The one profession that is never out of a job is a good doctor (second most job secure is a good cook).
However, while incompetent cooks are merely fired, incompetent doctors on the other hand, face perils ranging from having their license revoked to lawsuits. If their bungling actually kills the patient, doctors may even face frontier justice (e.g., thrown out the airlock sans space suit).
People might think it is romantic to go homesteading with just their spouse and kids on a remote planetary colony with no doctor or nuthin', right up to the point where they suffer a tooth-ache, broken limb, or a sudden attack of appendicitis. Ain't so romantic now, eh Jeremiah Johnson? Doctors are vital.
On near future solar system exploration ships a doctor will be indispensable. A Mars expedition could be out of range of a hospital for about 2.7 years.
And you will need multiple doctors on board a military spacecraft going into battle.
Doctors/Medics are never risked on any hazardous non-medical task or possibly dangerous environment. A first-in scout mission on a newly discovered planet could be in deep doo-doo if the doctor takes a stroll and is suddenly eaten by the Giant Trap-Door Spideroid(link trigger warning: spiders). The doc has to stay inside the ship, where it is relatively safe, no matter how much they are suffering from cabin fever.
The Patrol ship Starfire, Vegan registry,came into her last port at early morning. She made a bad landing, for two of her eroded tubes blew just as the pilot tried to set her down. She had bounced then, bounced and buckled, and now she lay on her meteor-scarred side.
Ranger Sergeant Kartr nursed his left wrist in his right hand and licked blood from bitten lips. The port wall of the pilot’s cubby had become the floor and the latch of its door dug into one of his shaking knees.
Of his companions, Latimir had not survived the landing. One glance at the crazy twisted angle of the astrogator’s black head told Kartr that. And Mirion, the pilot, hung limply in the torn shock webs before the control board. Blood rilled down his cheeks and dripped from his chin. Did dead men continue to bleed? Kartr didn’t think so.
Must get out and find the medico to look at Mirion. The pilot should not be moved until they knew the extent of his injuries—
Then Kartr remembered. The medico wasn’t around any more. Hadn’t been with them since three—or was it four?—planets back. The ranger shook his aching head and frowned. That loss of memory was almost worse than the pain in his arm. He mustn’t lose his grip!
Three planet landings back—that was it! When they had beaten off the Greenies’ rush after the ship’s nose blaster had gone dead on them, Medico Tork had gone down, a poison dart right through his throat.
(ed note: Pay attention to Ms. Linsky, she used to be a real-live military nurse)
I do, however, want to call his attention to a presumption he (Winchell Chung) has made, which I don't know is justified. Notably, that ships will carry doctors.
Why do I not know if this assumption is justified? Well, for a couple of reasons. First of all, because the vast majority of American warships do not have doctors aboard... they have Hospital Corpsman such as I once was. During WWII, hospital corpsmen aboard ships would even perform emergency appendectomies, usually on the mess deck (as Mr. Chung notes) using bent spoons as retractors. Talk about meatball surgery!
Hospital Corpsmen and their Army brothers, "Medics," receive initial training at "A School," an 18-week course. (You can also strike into the rate, as I did, but that's another discussion altogether). They receive ongoing OJT and "C Schools" throughout their career, as they go up in experience and rank. By the time a Corpsman / Medic has served a twenty year career, they may be qualified to receive the civilian designation of "Physician's Assistant," to practice medicine in the civilian field, under the supervision of a doctor.
Which brings me to my next point: advanced-practice nurses. With a master's degree, a nurse may become a nurse practitioner, a nurse midwife, a nurse anesthetist, and so forth. Again, these practitioners are nominally supervised by a physician (either an M.D. or a D.O.), but such supervision may be hundreds of kilometers away, here on Earth today.
So why would a ship prefer one of those options? A corpsman, as mentioned, receives an 18-week course, and is paid as an enlisted person. Nurses (the military only accepts baccalaureate prepared nurses; associates degree nurses are simply well-educated Corpsmen / Medics) are officers, and Doctors are officers who start service as O2 or O3 paygrades.
Plus, in space, it takes a long time to get anywhere. During that time, a corpsman who starts the voyage as an E4 may have hundreds of hours of available time to study advanced subjects, to work in simulation, and to advance in competence and paygrade. In essence, you're training your medical people during the time you're paying them to be there, anyway. And although you're paying them to be there, you're really hoping their skills won't be needed, so why not spend the time they might be reading romances on training, instead?
Additionally, there's the time to create the medical professional. I've mentioned a couple of times that Hospital Corpsman A School is 18 weeks long. Nursing school for a BSN is six semesters in most programs, followed by a year of practice as an RN, which then opens up MSN programs that can lead to advanced practice nursing in another four semesters or so. (The Doctor of Nursing Practice (DNP) degree is beginning to become popular, but I honestly know very little about it, or about the differences in scope of practice between DNP and MSN advanced practice nurses).
Physician's Assistant programs are likewise master's degree programs, but again, outside my scope of attention, so I don't know a lot about them. It seems to me that PAs have a very similar scope of practice to Nurse Practitioners, but I haven't really looked into it.
Both M.D. and D.O. (in the United States, at any rate) are three-year post-baccalaureate programs, which then also require internship and residency.
In short, a corpsman requires an initial investment in five or six months of training, while a PA or NP requires five or six years, and an MD or DO up to ten years before they're fully qualified to practice.
Consider also the state of expert systems aboard your ship. IBM has recently demonstrated Watson in an oncology role, with substantially higher correct diagnoses of cancer than human oncologists.
I suspect that future starships will mostly be crewed with people trained to render immediate, on-site first aid, to stabilize the victim, and get them into an auto-doc. The machine will then analyze the situation, display their analysis and reasoning to the Corpsman, ask for review / approval, and take whatever action is required once that approval is given.
There may be doctors aboard Capital ships or bases, but onboard a forward deployed cruiser? Corpsmen.
From Navy veteran and nurse JENNIFER LINSKY (2016)
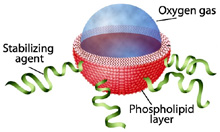
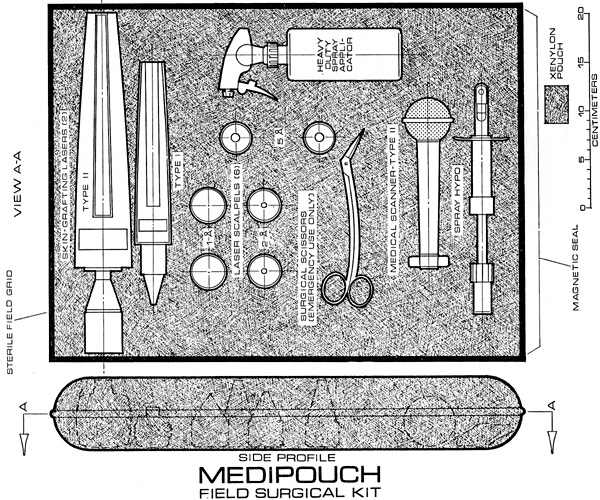
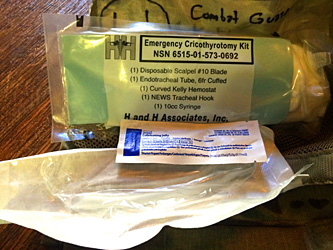
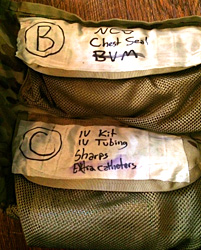
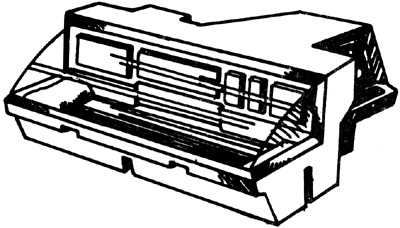
What's in the sickbay? What you'd expect: medical supplies, diagnostic equipment, maybe a sick bed or two, maybe a suspended animation cryo-freeze to put a seriously ill or injured crewperson on ice until the ship can make it to port. On a military ship, the sick bay may have its own separate life support system.
It might have the luxury of a surgical bed, or the doctor might have to make do with a table in the mess deck. (This is why there is a tradition on military ships for off-duty personnel removing their headgear while on the mess deck. It is a sign of respect for the crewmembers who have in the past, or may in the future, suffer and die there.) During combat, the mess deck become the emergency triage/operating room.
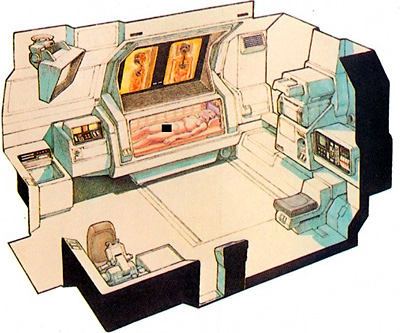
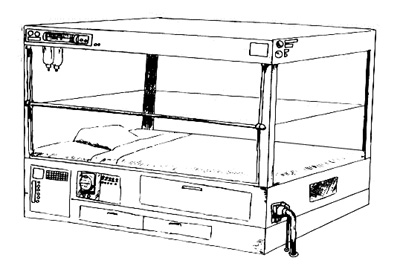
DOCTORS CABIN + SICKBAY
Unlike the other officers' cabins, which were fitted with more sophisticated equipment occupying much less space, Mercer's did not give much room for him to move. From the entry lock, the floor grill stretched ten feet to the curved plastic canopy that ran from below his feet to what was nominally the ceiling and gave, in the ship's present mode, a one hundred and eighty degree view of the inside of the outer hull, complete with structural members and brightly colored cable runs. The floor grill, which was just under three feet wide, separated two vertical tiers of bunks, eight on one side and five on the other. This was because the lowest one of the five was Mercer's, and he, being the doctor, needed much more than the twelve inches which divided patients' bunks.
A passenger unfortunate enough to come down with an infectious disease could be isolated from the living quarters and other patients, because the bunks were each fitted with an individual air supply and a hinged flap which sealed in the patient. Mercer did not suffer from claustrophobia, but he thought that any patient needing to spend more than a few days in one of those bunks would have to be kept under heavy sedation if he wasn't to blow his organic computer.
From LIFEBOAT by James White (1972)
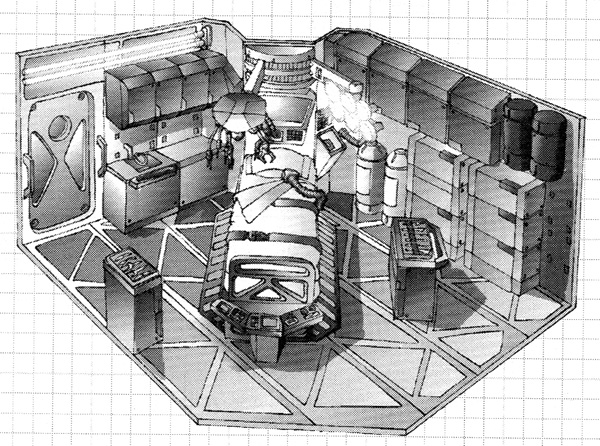
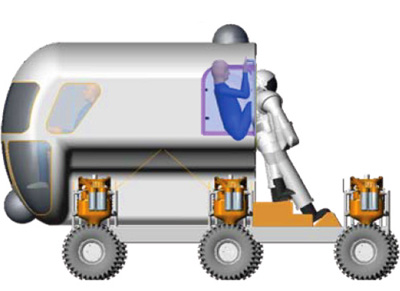
CEGA SICKBAY
CENTRALIZED EARTH GOVERNMENT AND ADMINISTRATION SICKBAY
Designed and drawn by Ghislain Barbe.
Cramped conditions are commonplace on a boat. A boat's sick
bay is thus a masterful arrangement of medical equipment. Everything
has a place. Symbols on cabinet doors identify what items
are to be kept inside. This allows medics to readily find items in
an otherwise unfamiliar sick bay.
Micro-gravity conditions create many challenges to traditional
medicine. Aside from combating muscle and bone degeneration,
space medics have to cope with fluid properties. Under gravity,
blood can be easily drained — not so in micro-gravity, where it
will float away. Suspended vacuum hoses scoop up the blood as
it leaves the patient before it can get into the equipment.
(ed note: Cot-Vee = Cargo Orbital Transfer Vehicle {COTV}, Pot-Vee = Personnel Orbital Transfer Vehicle {POTV})
"Okay, T.K., look at it this way. Those three hundred people in LEO Base can get back to Earth in less than an hour if necessary; we'll have lifeboats, so to speak, in case of an emergency. But out there at GEO Base, it's a long way home. Takes eight hours or more just to get back to LEO, where you have to transfer from the deep-space passenger ship to a StarPacket that can enter the atmosphere and land. It takes maybe as long as a day to get back to Earth from GEO Base— and there's a lot of stress involved in the trip." Hocksmith paused, and seeing no response from the doctor, added gently, "We can get by with a simple first-aid dispensary at LEO Base, T.K., but not at GEO Base. I'm required by my license from the Department of Energy as well as by the regulations of the Industrial Safety and Health Administration, ISHA, to set up a hospital at GEO Base." He finished off his drink and set the glass down. "If building this powersat and the system of powersats that follow is the biggest engineering job of this century, T.K., then the GEO Base hospital's going to be the biggest medical challenge of our time. It'll be in weightlessness; it'll have to handle construction accidents of an entirely new type; it'll have to handle emergencies resulting from a totally alien environment; it'll require the development of a totally new area of medicine— true space medicine. The job requires a doctor who's worked with people in isolated places—like the Southwest or aboard a tramp steamer. It's the sort of medicine you've specialized in. In short, T.K., you're the only man I know who could do the job . . . and I need you." John Curry, comptroller of Eden Corporation, looked disturbed as he scanned the sheet of budget figures Tom had submitted to him several days before. "Doctor, I didn't realize you'd have to set up a complete hospital at GEO Base." "We'll need a complete trauma center, as well as an intensive care unit," Tom explained. "I'll also have to be prepared to handle something more than runny noses; I'll need a pathology lab and a blood lab. I'll need radiology equipment because I can't send an employee back to the Jornada with broken bones I don't know about; the accelerations of return and atmospheric entry could kill a person if we didn't know where the break was and take steps to protect him against acceleration. If we could let him come back to Earth at all. We might have to let him heal up there." Curry drummed his fingers on his desk top while he studied the budget sheet once again. "But a ten-bed hospital? Isn't that rather large for a construction-site operation, Doctor?" "That's fewer beds per thousand people than the state of New Mexico has right now—and you know this state's desperately short of hospital beds," Tom told him bluntly. "I'm going to be twenty-two thousand miles away with no possibility of getting help in an emergency and no way to get an injured or sick person back to the ground in less than a day. And those time estimates are under the best conditions with Pot-Vees and StarPackets on hand and ready to move." "The cost of the equipment doesn't bother me," Curry went on. "We'll work that out so it's a capital expense properly written off in a way that'll keep the IRS happy and the government auditors pleased. What's difficult is the cost of getting the equipment there." (ed note: every gram counts) "I know," Tom admitted. "That's why I've tried to choose equipment that weighs as little as possible. In some cases I've specified new equipment that has yet to be tried and proved. I've got to take certain risks, however, because I understand the costs of getting the equipment to GEO Base as well as the costs in terms of electrical and cooling energy to operate it once it's there." He was glad that Dan Hills had been so helpful in going over the engineering aspects of his GEO Base clinic. Things he took for granted on Earth became serious problems at GEO Base. For example, he had to consider thermal efficiency of equipment, since the heat load of GEO Base had to remain in balance. Calories coming in had to balance calories going out; otherwise, equipment heat losses would literally burn the place up. The drawings of the GEO Base hospital already showed the hex module festooned with heat radiators. "I wish there were some way to beat some of these lift costs," Curry remarked, shaking his head. "When we get rolling on the two-per-year production phase, that won't be so important. But the start-up costs of this pilot-plant phase are all out of proportion." Tom thought about how he might have to handle things at the H-Bar-S Ranch if there were a number of injured or sick people and no way to get equipment in or patients out. It was a problem he had faced before. "Uh, John, maybe I can skimp a few things to start with if have outstanding communications links." Curry began to nod slowly. "I think I see what you mean, Doctor. GEO Base will have a communications capability with a large number of broad-band, high bit-rate channels. Uh, would a high bit-rate computer link and an interactive video system help?" "That's what I was thinking about," Tom acknowledged. "What could you eliminate if you had good communications capabilities?" "Some of the analysis equipment. If I have rapid access to one of the medical computer networks, I could squirt raw data to lab facilities here on Earth. I could also eliminate most of that microfilm medical data I specified, because then I could tie in with any computerized medical library here ... or I could go interactive on a video channel with one or more specialists if I ran into something where I needed consultation." Curry reached down into his desk, pulled his terminal to desk-top level, keyed it, and looked at the display. "We can set you up with any number of nets. How about GALEN—General Analytical and Library Electronic Network?" "Never heard of it." "One of the best medical nets going, it says here." Tom had worked out eight basic medical areas he would have to be prepared for. First, there were the usual job-related injuries that were physical: cuts, bruises, burns, abrasions, and even severed limbs. Then there were the pathological aspects, basically public health measures to block entry of infectious bacteria and viruses into space facilities as well as to counteract them when they did sneak in, as they always managed to do. He also had to be prepared for what he termed the congenital afflictions—appendicitis, tonsilitis, cholecystitis, toothaches, etc. There would also be stress-related illnesses manifesting themselves in hypertension, cardiac problems, and psychosomatic conditions—plus psychological problems caused by isolation and phobias such as the one Ross Jackson had mentioned with the Gemini astronaut. He had to keep watch for biochemical problems that might be exacerbated or brought on by dietary deficiencies, glandular imbalances, and so forth, plus the medical problems created by social interaction, because there were certain to be fights and alcoholism, and even some drug abuse, strict as the preflight inspection might be. Tom knew enough about human nature to realize somebody would either manage to sneak the stuff up or cobble together a vacuum still. But the biggest problems were still environmental, the medical aspects of the space environment itself. At GEO Base, he knew he couldn't take a lot of things for granted, earthly things like food, water, temperature, atmosphere, and radiation. These were items that really had him worried. Four people were jammed into First-Aid when he arrived, and the place was filled with a pink mist. All four people wore pressure suits, but three were without helmets. The exception was a short, stocky person whose utterly relaxed position, afloat in the compartment, spelled "unconscious" to Tom. "Get that off!" Tom snapped to a young woman who was holding the man by his pressure helmet. "What happened here?' Then he saw that the right leg of the man's pressure suit terminated at the lower end of the calf, just above the ankle. So that was the source of the pink mist. "Fred was working on the power-control junction and must have had a suit radio failure," the young woman remarked. There was no panic in her voice. "Some yo-yo was trying to mate the attach points of another submodule, and he didn't see Fred's leg in the way. When I saw it and yelled, Fred didn't hear me. His radio must have been out." The man's foot was sheared through just above the ankle, and it had not been a clean severance. Somebody had acted fast out there, and the conipartmentation of the pressure suit had saved the man. A rough tourniquet of electrical cable had been wound around his leg, the only thing that had prevented the pressure in his suit from pumping all his blood out into vacuum. Nonetheless, he had lost a lot of blood. Moving in a hurry in weightlessness was difficult and bordered on the impossible because Tom wasn't used to it. Several times he pushed off too robustly and ended up banging hard against bulkheads or cabinets. The equipment he removed from cabinets wouldn't behave itself. Fitzsimmons was in shock, and it was important that Tom get oxygen and stimulants into the man immediately, but the hose on the oxygen mask wound itself all over the place. Finally, with Lucky Hertzog's help, he managed to get the oxygen mask securely in place. There was no way that an IV was going to work, Tom discovered. Without gravity, it wouldn't drip. He thought of injection, then discovered he couldn't get the air bubbles out of the syringe in the usual manner. He ended up swinging it at the end of his arm and squirting most of the injection into the compartment before he felt it had been deaerated enough to prevent an embolism. Getting the IV working was strictly a lash-up, and he didn't have time to be neat. He had to start lactate of Ringer going right away, followed by whole blood—if there was any—followed by closing or cauterizing the severed blood vessels that, in spite of the tourniquet, were still seeping. He called in one of the men from the passageway and instructed him on how to inject the IV solution gently and slowly into Fitzsimmons' arm. No whole blood was available in the First-Aid Center. Tom cursed himself for not specifying that there be some. It was, therefore, vitally important that he tie off the blood vessels as quickly as possible. When Torn couldn't find any sutures in the cabinets, he yelled for the remaining man waiting in the passageway. "You, get up to my quarters and bring back my flight kit. I don't know the compartment number—ask a steward. And hurry!" After ten minutes passed and the man had not returned, Tom was in a bind. He had to stop the bleeding. "I've got to cauterize! Is there a welding torch around here?" "Nobody in his right mind would do oxyacetylene welding here," Lucky told him. "If I don't, this man's going to die from blood loss!" "How about an arc welder?" "Get it in here!" Tom didn't know how he was going to cauterize the stump of a leg with an electric arc welder, but he would try to figure something out. Unfortunately, there wasn't an arc welder within three hex modules of First-Aid. Tom didn't panic, but he was slowly coming to the conclusion that his worst fears would be realized. He was going to lose this man because he hadn't been able to assess the medical requirements of a space facility accurately. Lucky Hertzog released Fitzsimmons' head and moved toward the compartment door, maneuvering easily in zero-g. "Where are you going?" Tom asked. "You've got to seal that stump, right?" "Right, but—" "I'm going over to the beam builder three modules away. I'll bring back enough activated epoxy to cover that whole stump." And she was gone. But the man returned with Tom's bag before Lucky did. Tom kept packaged sutures and needles in his kit, along with the necessary surgical tools. He always tried to go prepared to handle emergencies, a habit born from his life in the Southwest, where towns and doctors were far apart. Tom was in the process of tying off arteries when Lucky Hertzog floated in, both hands full of a lump of curing epoxy. "How long before that cures?" "About fifteen minutes, Doc. It's got maybe ten minutes' working life left." "Okay, I can get these arteries tied off by then. Stand by." But doing so wasn't as easy as he had thought. Blood spurted everywhere. It was almost impossible to keep the working area clear of blood, which formed drops and globules, its surface tension making it creep along the exterior of every object it touched. But he managed to get the main arteries tied, then formed a base to the stump with the glob of epoxy. The procedure worked. The blood flow stopped, and Tom was able to remove the tourniquet. It hadn't been sterile, and it hadn't been neat, but Fitzsimmons was still alive. Then his heart stopped in shock from general loss of blood. "CPR!" Tom snapped. He quickly discovered CPR wouldn't work in weightlessness. When he punched down on Fitzsimmons' chest, he and Fitzsimmons flew apart. Lucky quickly jammed Fitzsimmons' body into a locker along one side of the compartment and jammed herself in with him. With her back against one side of the locker and his against the other, she began CPR. "Spell me," she gasped to Tom after about five minutes, during which time he had been trying to get the leads of the defibrillator untangled. One of her men moved in and took over, leaving Tom to his struggle. But between Lucky Hertzog and her two workers, they managed to get Fitzsimmons' heart going again without the need for Tom to defibrillate—a risky business in the metal-walled compartment.
From SPACE DOCTOR by Lee Correy (G. Harry Stine) 1981
ORBITAL HOSPITAL
In May 1967 I was in Dallas to attend the first conference on the commercial uses of space—including tourism.
Barron Hilton gave a talk on the Hilton Orbiter Hotel,
which he hopes to see in his lifetime. Space tourism is
going to be a major industry in the twenty-first century.
Another tremendously important use of space stations
will be for medical research; one paper given at Dallas
discussed the engineering problem of a hospital in orbit.
Which brings a poignant memory to mind. The last letter
I ever received from that great scientist Professor J. B. S.
Haldane was written when he was dying of cancer and in
considerable pain from his operations. In it, he said what
a boon the weightless environment of a space hospital
would be to patients like himself—not to mention burn
victims, sufferers from heart complaints, and those afflicted
with muscle diseases. I am convinced that research in
space will open up unguessed regions of medical knowledge
and give us a vast range of new therapies. So I get pretty
mad when I hear ignorant but well-intentioned people
ask, “Why not spend the space budget on something useful
—like cancer research?”
When we do find a cancer cure,
part of the basic knowledge will have come from space.
And ultimately we will find even more important secrets
there: perhaps, someday, a cure for death itself…
DRAINING an infected abscess on Earth is a straightforward procedure. On a spaceship travelling to the moon or Mars, it could kill everyone on board.
Blood and bodily fluids cannot be contained in zero gravity, which means there is currently no way to perform surgery in space without contaminating the cabin. This makes an extended stay problematic, says James Antaki at Carnegie Mellon University in Pittsburgh, Pennsylvania. “Based on statistical probability, there is a high likelihood of trauma or a medical emergency on a deep space mission,” he says.
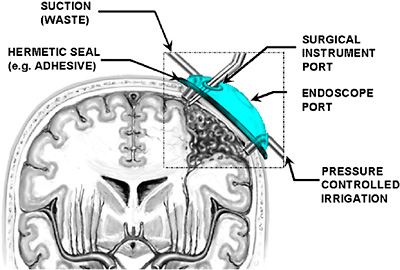
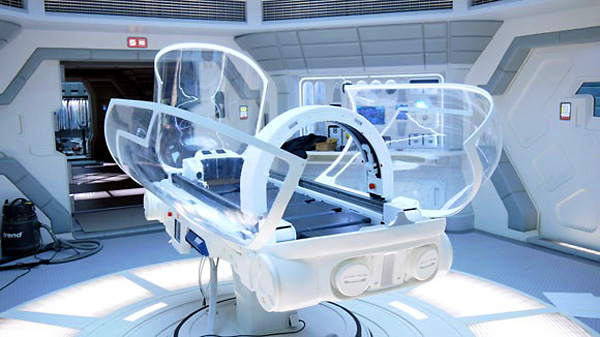
Antaki is part of a team of US researchers developing an astro-surgical tool that could help. The Aqueous Immersion Surgical System, or AISS, is a transparent box that creates a watertight seal when it is placed over a wound and pumped full of sterile saline solution, says George Pantalos at the University of Louisville in Kentucky.
The saline solution is held under pressure inside the AISS to prevent blood from seeping out of the wound. Airtight holes allow surgeons to access the submerged wound using handheld and orthoscopic instruments.
By varying the pressure within the AISS, the device could also be used to siphon up and recycle blood. “You won’t have a blood bank in space, so if there is bleeding you want to save as much blood as you can,” says James Burgess, also at Carnegie Mellon, who came up with the concept.
Imagine a medical emergency on a flight to the moon, an asteroid or Mars—it may not be as catastrophic as the crisis in the film Gravity, but perhaps an astronaut is bleeding. Surgery can always be challenging, but it would be even more so in microgravity, because blood droplets can float, potentially obscuring a caregiver’s field of view. Now researchers have tested a novel way to potentially control bleeding during surgery in space by isolating wounds under transparent watertight domes filled with fluid.
For the past three decades scientists have explored ways surgery could be performed in space. The main problem is that sans gravity, blood could drift into the eyes, nose and throat as well as potentially spread disease among the crew. It could also splatter inside spacecraft cabins and perhaps muck up vital electronics. In 1984 researchers reported one system that would essentially wrap plastic bags around wounds to attempt to control bleeding, and another tested in 1993 would fully enclose patients in rigid transparent boxes. Surgeons could stick their hands and tools into either containment system to operate. A critical shortcoming of both strategies was that blood could paint the container walls and obscure the view.
Neurosurgeon James Burgess at Allegheny General Hospital in Pittsburgh came up with the idea of placing a transparent dome over a wound and then filling it with fluid such as saline solution. The fluid’s pressure could slow and even stop bleeding until a surgeon can seal the wound. "A hydrostatic pressure is like a force field—it's what a science fiction writer might imagine," says researcher James Antaki, a biomedical engineer at Carnegie Mellon University. "The idea is simultaneously revolutionary and common sense, the definition of an inventive solution to the problem, like the upside-down ketchup bottle."
Ports in the dome could allow insertion of conventional or endoscopic surgical tools. Moreover, "a suction tool can also be directed to where the bleeding is to clear the surgeon's field of view," Pantalos says.
Although Burgess originally came up with the idea to help keep delicate tissues from drying out during brain and spinal surgery, along with control profuse bleeding that can happen during operations, Pantalos and his colleagues reasoned this Aqueous Immersion Surgical System (AISS) could also help in microgravity. "We have begun to feel satisfied that the concept is applicable in almost in any surgical situation—on Earth or in space," Burgess says.
The AISS poses a number of tricky challenges. For instance, the researchers want to maintain constant pressure under the dome when suctioning blood away by pumping in fluid at roughly the same rate—otherwise pressure drops could worsen bleeding whereas increases could push fluid into the body and cause swelling.
It has been estimated that there will be one surgical emergency every 2.4 years on a mission to Mars. T. Trapp/BJS Surgery, CC BY-SA
Earlier this year, it was reported that an astronaut in space had developed a potentially life-threatening blood clot in the neck. This was successfully treated with medication by doctors on Earth, avoiding surgery. But given that space agencies and private spaceflight companies have committed to landing humans on Mars in the coming decades, we may not be so lucky next time.
Surgical emergencies are in fact one of the main challenges when it comes to human space travel. But over the last few years, space medicine researchers have come up with a number of ideas that could help, from surgical robots to 3D printers.
Mars is a whopping 54.6 million kilometres (33.9 million miles) away from Earth, when closest. In comparison, the International Space Agency (ISS) orbits just 400 kilometres above Earth. For surgical emergencies on the ISS, the procedure is to stabilise the patient and transport them back to Earth, aided by telecommunication in real time. This won’t work on Mars missions, where evacuation would take months or years, and there may be a latency in communications of over twenty minutes.
As well as distance, the extreme environment faced during transit to and on Mars includes microgravity, high radiation levels and an enclosed pressurised cabin or suit. This is tough on astronauts’ bodies and takes time getting used to.
We already know that space travel changes astronauts’ cells, blood pressure regulation and heart performance. It also affects the body’s fluid distribution and weakens its bones and muscles. Space travellers may also more easily develop infections. So in terms of fitness for surgery, an injured or unwell astronaut will be already at a physiological disadvantage.
But how likely is it that an astronaut will actually need surgery? For a crew of seven people, researchers estimate that there will be an average of one surgical emergency every 2.4 years during a Mars mission. The main causes include injury, appendicitis, gallbladder inflammation or cancer. Astronauts are screened extensively when they are selected, but surgical emergencies can occur in healthy people and may be exacerbated in the extreme environment of space.
Floating intestines
Surgery in microgravity is possible and has already been been carried out, albeit not on humans yet. For example, astronauts have managed to repair rat tails and perform laparoscopy – a minimally invasive surgical procedure used to examine and repair the organs inside the abdomen – on animals, while in microgravity.
These surgeries have led to new innovations and improvements such as magnetising surgical tools so they stick to the table, and restraining the “surgeonaut” too.
One problem was that, during open surgery, the intestines would float around, obscuring view of the surgical field. To deal with this, space travellers should opt for minimally invasive surgical techniques, such as keyhole surgery, ideally occurring within patients’ internal cavities through small incisions using a camera and instruments.
A laparoscopy was recently carried out on fake abdomens during a parabolic “zero gravity” flight, with surgeons successfully stemming traumatic bleeding. But they warned that it would be psychologically hard to carry out such a procedure on a crew mate.
Bodily fluids will also behave differently in space and on Mars. The blood in our veins may stick to instruments because of surface tension. Floating droplets may also form streams that could restrict the surgeon’s view, which is not ideal. The circulating air of an enclosed cabin may also be an infection risk. Surgical bubbles and blood-repelling surgical tools could be the solution.
Researchers have already developed and tested various surgical enclosures in microgravity environments. For example, NASA evaluated a closed system comprising a surgical clear plastic overhead canopy with arm ports, aiming to prevent contamination.
When orbiting or settled on Mars, however, we would ideally need a hypothetical “traumapod”, with radiation shielding, surgical robots, advanced life support and restraints. This would be a dedicated module with filtered air supply and a computer to aid in diagnosis and treatment.
Robots and 3D printing
The surgeries carried out in space so far have revealed that a large amount of support equipment is essential. This is a luxury the crew may not have on a virgin voyage to Mars. You cannot take much equipment on a rocket. It has therefore been suggested that a 3D printer could use materials from Mars itself to develop surgical tools.
Tools that have been 3D printed have been successfully tested by crew with no prior surgical experience, performing a task similar to surgery simply by cutting and suturing materials (rather than a body). There was no substantial difference in time to completion with 3D printed instruments such as towel clamps, scalpel handles and toothed forceps.
Robotic surgery is another option that has been used routinely on Earth, and tested for planetary excursions. During NEEMO 7, a series of missions in the underwater habitat Aquarius in Florida Keys by NASA, surgery by a robot controlled from another lab was successfully used to remove a fake gallbladder and kidney stone from a fake body. However, the lag in communications in space will make remote control a problem. Ideally, surgical robots would need to be autonomous.
There is a wealth of research and preparation for the possible event of a surgical emergency during a Mars mission, but there are many unknowns, especially when it comes to diagnostics and anaesthesia. Ultimately, prevention is better than surgery. So selecting healthy crew and developing the engineering solutions needed to protect them will be crucial.
There are all sorts of drugs in science fiction, some medical and some not.
Keep in mind that all drugs are poisons, and all poisons are drugs. The only distinguishing feature is the dosage. One aspirin can cure a headache but when your child eats a whole bottle you have to rush them to the emergency room to get their stomach pumped.
In my personal opinion, medications that would make the owner of the drug patent rich beyond the dreams of avarice would include a cure for male-pattern baldness and a diet pill that would allow you to pig-out on whatever food you wanted and still look buff and cut like a Hollywood star.
If you get fancy one can do intradermal injections via air with a jet injector (though Doctor McCoy calls it a hypospray). In Isaac Asimov's The Caves of Steel they use "hypo-slivers", pointy shards of solid drug that are inserted under the skin like a medical splinter of wood (science-fictional but probably impractical).
Topical creams are usually for delivering medicine to the skin not through the skin, since said skin is remarkably good at preventing drugs from penetrating. The few drugs that can penetrate are sometimes administered by a transdermal patch. Thankfully, one of the drugs that can penetrate is dimenhydrinate, an anti-nausea drug. NASA astronauts always stick on one of these when they get into a space suit for an EVA. This prevents both nausea and the danger of an astronaut drowning in a fishbowl full of their own vomit.
And of course assassins spend a lot of time inventing surprising and unexpected ways to get poison into their victims.
SPACE PHARMACY
In space, no one can hear you sneeze. But if an astronaut does catch the flu, it can be a major problem. With the nearest Walgreens several hundred kilometers away, every medication an astronaut could possibly need on a space mission must be packed beforehand. It makes designing a pharmacy for space extremely complicated.
On top of that, of course, space itself poses potential medical issues. That extreme environment is known to warp the human body, shift fluids, and shrink bones, among other things. But microgravity can also affect how medications are metabolized, potentially making drugs less effective or even toxic.
Yet, despite 60 years of humanity sending individuals to space, there has been alarmingly little research into how meds work differently off-planet. While self-medicating in space has been common, there aren’t great records of who took what, when they took it, and how it did or didn’t help. There is some evidence that certain meds can be less potent in space and radiation may even degrade medications—but really, experts just aren’t sure.
“If you go to the doctor, there are basically three things they can do for you,” Dr. Virginia Wotring, a professor at the International Space University in Strasbourg, France, told Ars. “They can perform surgery, they can advise you to change your behavior—you know, stop smoking or whatever—or they can give you a medication. Which means [for space travel], a physician's best tool is going to be the medication kit… This is something that merits attention, that astronauts deserve to know.”
The great unknowns
If all the careful preparation NASA astronauts Dog Hurley and Bob Behnken did recently to ride to the International Space Station in the middle of a pandemic doesn’t give it away, astronauts already abide by extremely strict health regimens. Even in healthier times, they quarantine for weeks before launches. Not much of their behavior needs changing. Surgery in space carries tremendous risk and luckily has never happened. Medication represents the best choice for out-of-this-world treatment by default, making the lack of research around the topic increasingly curious.
“At this point, we're making an assumption that medications get absorbed and distributed to tissues and metabolized and excreted mostly the same way in space,” Worting said. “That might not be the truth.”
For example, a 2014 study measured sleep deprivation in astronauts aboard the International Space Station (ISS) and the drugs they took to get to some rest, such as zolpidem, brand name Ambien. The researchers, some from Harvard Medical School, found the astronauts often took a second dose in the middle of the night, presumably because the first dose didn’t provide enough relief.
But multiplying medications can mean increasing risk of side effects, or in the case of Ambien, potential grogginess during an emergency. Imagine trying to respond coherently after waking suddenly to a warning alarm while being “ambientoxicated.”
To better understand the mysteries surrounding what drugs would be effective for long-term stays in space, Wotring designed an iOS app that six crewmembers aboard the ISS volunteered to use for logging their meds in 2017. Every time they took a pill, the astronaut would record the drug name, the dose, the indication for taking the medicine, and whether they thought it worked, plus any side effects.
Wotring and her co-author LaRona Smith, a clinic administrator at Johnson Space Center, collected 5766 records of medication use—around 38 times more than the records from all previous space flights combined. “We were expecting more data,” Wotring said. “I was completely blown away when we saw how much data were coming in.” The results were published in the journal Aerospace Medicine and Human Performance this past January.
Medication use, on average, was somewhat more than on Earth, Wotring and Smith found. Sleep was the most common reason for taking a drug, but mild painkillers like ibuprofen were also frequently swallowed. “Most medications were considered partially effective,” they wrote. Even though the app apparently suffered from usability issues, causing the study to conclude early (insert Apple snark here), Wotring says NASA is in the process of adopting a similar protocol so they can better track their cosmonaut’s drug needs. Until then, a lot of unknowns remain.
“We know that there are physiologic changes to the human body in spaceflight. It makes sense that the effects of medications may be different in the altered physiology of the astronauts,” Dr. Tina Bayuse, lead pharmacist at Johnson Space Center Pharmacy Operations, said in an email. In 2002, she became the lead pharmacist for NASA’s first and only pharmacy.
“Changes in gastric motility may impact the absorption of medications,” Bayuse explained. “Fluid shift alterations may influence how medications are distributed or metabolized. The outcome of any of the known physiologic changes may result in medications that cause more side effects or are less effective.”
Medicine on Mars
Although this has been identified as an area for more research and studies like Wotring and Smith’s have begun, that work may have to happen relatively quickly given today’s space ambitions. To fully prep for future space flights, including lunar stations or long trips to Mars, we need a lot more data first, according to Rebecca Blue, a research collaborator at the Aerospace Medicine and Vestibular Research Laboratory at The Mayo Clinic in Arizona. The reason we know so little about drug metabolism in space, Blue told Ars, is because humans haven’t ventured too far from Earth yet, and tight budgets have prioritized other aerospace research.
“When we go to the Moon or Mars for longer and longer durations, we may not have this capability to provide, resupply, or replenish stock,” Blue told Ars in a call. “Suddenly, we have to start thinking about that.”
Another issue is that the quality of little research done on space and drugs thus far frankly isn’t great. Like Wotring’s dose tracking experiment, studies usually have small sample sizes or lack controls. Going to space is also incredibly expensive, so it’s difficult to repeat experiments or gather much data. To get around this, a lot of research is performed on rodents or in “analog” environments—not with human volunteers in outer space itself.
For example, a NASA-funded study published in April tried to simulate how drug metabolism works in space by exposing male Wistar rats to X-ray radiation and collecting their urine after being injected with methamphetamine. It may sound strange to give rats the same stuff from Breaking Bad instead of a drug astronauts actually use, but this was medical-grade speed, which does have health applications.
More importantly, how meth is metabolized in rats has been well-studied, making it easier to trace how the stimulant moves through the body. The amount of radiation some rats were exposed to was “approximately what one would be exposed to on a round trip to Mars,” Dr. Michael Hambuchen, one of the study’s lead authors, explained in an email. Others got a dose equivalent to a “round trip with a 10 year stay on the planet’s surface.” Rats not exposed to radiation were used as controls.
Ultimately, it didn’t seem like the radiation had any impact on the pharmacokinetics of the drug—a good sign for astronauts who might take similar stimulants like Adderall. But more research is still needed.
“The main weakness of this approach is the acute radiation exposure rather than a gradual irradiation over time, as would occur in human astronauts,” said Hambuchen, who is an assistant professor at the Marshall University School of Pharmacy. “It’s bizarre how well worked out and described methamphetamine pharmacokinetics are in rats … While I stand by my rationale for using meth as a probe in this study, it may be beneficial to repeat this experiment with drugs in the NASA spaceflight formulary.”
Analog space environments have been used for studies involving humans, too. A study published in Clinical Pharmacology in 2005 described six patients given ciprofloxacin, a common antibiotic, while under the effects of simulated microgravity at a hospital in Gainesville, Florida. Compared to blood samples in normal gravity, plasma concentrations of ciprofloxacin were “almost identical,” although the results suggested tissue penetration of the drug might be slightly impaired in microgravity. In other words, not a very worrying difference.
To make these volunteers feel like they were in space, the researchers used a widespread technique called antiorthostatic bed rest (ABR). The way ABR works is pretty simple: patients lie in a hospital bed for days or even weeks with their heads down at a 6° to 12° angle (fun!). This, of course, rushes fluid from the legs to the brain, which is also sort of what happens in space.
However, while a 2016 review in Applied Physiology highlighted the strengths of this experiment design, it noted ABR is “probably not a true simulation of space flight.”
“When we are exposed to the normal gravitational force of the Earth, as you're standing or sitting upright, the fluid in your body is pulled down,” Blue said. “However, when you go into a microgravity environment—we call it a gravitational gradient—that pull of the fluid down towards your legs and your feet goes away. And so, as a result, the fluid redistributes.”
This sounds alarming, but it’s not life threatening. Astronaut bodies eventually do adjust to microgravity, an ambiguous condition called “space normal.” Still, we aren’t entirely sure if this fluid redistribution changes the way the body absorbs drugs, let alone other space-related variables like radiation, disrupted circadian rhythms, or the thickening of artery walls.
“It's measurably different from Earth, but there's not necessarily anything bad about it. It's normal for space,” Wotring said. But she noted that aerospace pharmacologists have to account for this change. “One of our concerns is if you changed blood volume by any significant number, well, do you need to change the dose of a drug? We don't know.”
Blue also noted that just taking medications in and of themselves is not without risk. “It's very hard to tease out reality when we don't have a perfect analog or the perfect ability to do dedicated controlled research studies during spaceflight,” she said.
Bringing drugs to space
So after all this, how do you decide what drugs to pack for Saturn’s moons? Since 1977, the World Health Organization has kept a growing list of “Essential Medicines” designed to meet the most important health needs of any population. It works as an excellent guide for developing nations to know what to keep stocked. But the current tally is 433 medications—you can’t bring all these aboard a spaceship, as the added weight would make a big difference.
NASA has narrowed down what ends up in their pharmacopeia. “For the most part, the medications we pack for our current missions are for common issues like congestion, headache, or motion sickness,” NASA’s Bayuse said. “Medications needed that provide a smaller footprint, don’t require special storage, or that can cover multiple indications are part of the consideration for inclusion into the medical kit.”
For example, if one medication calls for a higher dosing frequency to treat an indication—say, three times a day—and another in the same class for the same indication only once per day, NASA would consider the medication that needs to be taken less.
A 2016 FOIA request from NASA revealed some of what’s in the medicine cabinet onboard the ISS. Caffeine, of course, makes the cut, but so did modafinil, an alertness drug used to treat narcolepsy. If you need help dozing off instead, there’s melatonin and Ambien. If you’re having trouble relieving yourself, there’s Dulcolax, a stool softener, and Flomax for urination, or Imodium, an antidiarrheal med, if you require the opposite. To treat stomach issues, there’s Pepto Bismol, Prilosec, and other drugs for nausea and altitude sickness.
For allergies, there’s Allegra, Benadryl, and Claritin, plus epinephrine pens and pseudoephedrine, a decongestant. For pain, there’s everything from acetaminophen to hydrocodone to aspirin to ketamine, not to mention topical anesthetics like lidocaine. There’s a whole suite of antibiotics, from azithromycin to tobramycin, plus valacyclovir, for treating viruses like herpes.
Don’t forget the albuterol inhalers, eye drops, antifungal tablets, carbamide peroxide for earwax removal, several classes of steroids and hormones, as well as drugs for seizures, high blood pressure, and plenty more. There are even drugs to treat mental health, including antidepressants like Zoloft and Effexor, plus Valium for anxiety.
All that is just for the small crew aboard the ISS, however. This list could change for longer missions to the Moon and beyond. NASA is already thinking about what to add or throw out. “Exploration missions have and will require us to re-evaluate what is part of the medical kit in the future,” Bayuse said.
Medication stability
Longer missions bring more variables to how drugs work differently in space, including expiring faster. “Typically what we purchase and what is approved by the FDA or the equivalent European organizations has a 24 month shelf life,” Wotring said. Unfortunately, it takes about 36 months to get to Mars, which could be a major issue. It’s not like astronauts can get a new shipment of Vicodin.
“The stability of medications as a result of the spaceflight environment is largely unknown,” Bayuse said. “There has been some evidence that suggests that some medications may degrade [in space] before the listed manufacturer expiration date. Unfortunately, there have been some issues highlighted with those studies, such as not having ground controls to compare the results to, confounding variables and limited sample sizes hindering the reproducibility of the results.”
“Currently we do not have enough data to fully characterize what those results mean or how the care of our astronauts may need to be adjusted, if at all,” she added.
If some medications degrade and simply become useless, it could be a relief. In other cases, disintegrating drugs could create concentrations of toxic chemicals. “Tetracycline antibiotics are the poster child for this,” Wotring said. Tetracycline antibiotics are used to treat everything from syphilis to malaria to anthrax infections. But when they expire, tetracyclines seem to degrade into chemicals that cause kidney failure according to studies in past decades. (Doxycycline is one tetracycline antibiotic included on the ISS. Others, such as amoxicillin, may not have this issue.)
If stored correctly, some meds will work for years, even decades after expiration. But space is a different environment and some early evidence suggests the rate of decay is faster off-planet. A 2011 analysis published by the American Association of Pharmaceutical Scientists examined 35 drugs that had been stored on the ISS for 28 months. The meds came in different forms, including pills, creams, and liquids and the researchers also used ground controls to ensure accuracy.
“The rate of degradation was faster in space than on the ground for many of the medications,” the authors wrote, noting that drugs like promethazine and dextroamphetamine (Adderall) were especially susceptible to these changes, perhaps because they are light sensitive. Space radiation, excessive vibrations and abnormal gravity may also play a role.
All of this again ties into a massive lack of research. There’s just so much we don’t know about how drugs work in space. For now, that hasn’t been a huge issue, but it’s something NASA and other exploration agencies will need to consider sooner than later if we want to spread out from Earth.
“We’ve been able to manage the uncertainties of medication stability and effectiveness with routine resupply and crews that have been living and working in the spaceflight environment for a year or less,” Bayuse said. “As we transition to exploration missions where resupply is not certain and crews will be away for longer than a year, providing safe and effective pharmacy care will be more challenging.”
Improving pharmacies in space has broad implications for healthcare on the ground, too, Bayuse said. Innovations and new insights into the mechanisms of pharmaceuticals under extreme conditions could translate to better medicine on Earth, just like many aerospace innovations have improved our lives.
Ultimately, we may even discover that the issues with medication stability and how drugs are metabolized in space is a relatively minor issue with easy fixes. But until we have more data, it’s difficult to say.
“We may, through further study, find that this isn't as big of an issue,” Blue said. “I don't want to make it sound like I'm unnecessarily raising alarm bells because the truth is, we just don't know.”
In preparing this study of drug themes in science fiction, I have employed the following categorical designations:
Drugs as Euphorics: Drugs that give pleasure in simple unstructured ways, through release from depression and tension, much as alcohol does in our society (though alcohol is not strictly speaking a euphoric, of course).
Drugs as Mind Expanders: Drugs that provide "psychedelic"
visions of other times or places or that offer a sensation of oneness
with the cosmos as a whole; analogous to LSD in our society.
Drugs as Panaceas: Drugs which, through tranquilizing or
neutralizing effects, calm the mind without necessarily inducing
euphoria.
Drugs as Mind Controllers: Drugs that enable one entity to
limit or direct the activities or desires of another; analogous to
brain-washing, and generally associated with totalitarian activities.
Drugs as Intelligence-Enhancers: Drugs which have the specific
property of extending or amplifying the rational processes of the
mind.
Drugs as Sensation-Enhancers: Drugs whose effects are achieved
through amplified or extended bodily sensation-response, perhaps analogous to marijuana in our society.
Drugs as Reality-Testers: Drugs which permit the user to
penetrate the "real" realities beyond the surface manifestations of
daily life.
Drugs as Mind-Injurers: Drugs used as weapons in biochemical
warfare, aimed at the mind.
Drugs as Means of Communication: Drugs that have the specific property of opening hither to unknown channels of communication
between minds.
Two distinct attitudes toward the use of mind-related drugs
have manifested themselves in science fiction.
One is cautionary:
that any extraordinary indulgence in extraordinary drugs is likely to
rot the moral fiber of the user, leading to lassitude and general decay of the individual or of society, and ultimately, perhaps, aiding
the establishment of a totalitarian order.
The other is visionary and
Utopian: that through the employment of drugs mankind can attain
spiritual or psychological powers not ordinarily available, and by so
doing can enter into a new and higher phase of existence.
Author: Slesar, Henry
Title: I remember oblivion
Journal: Fantasy and Science Fiction, Vol. 30, No. 3, 36-43
Publisher: Mercury Press, New York
Date: March 1966
Format: Short story
Descriptor: Drugs as mind-controllers
Annotation: A technique has been devised for literal brainwashing of
criminals, i. e., the total eradication through chemotherapy
of memory, and the reconstruction, using drugs and "narcohypnosis," of a new non-criminal personality within the existing body.
The narrative cuts from the conversation of two scientists using the
technique to the s tream-of-consciousness of a rehabilitated criminal
who, breaking through his conditioning, regains access to his memories
and commits suicide in his guilt.
Author: Heinlein, Robert A.
Title: The Puppet Masters
Publisher: Doubleday & Co., New York
Pages: 219 pp.
Date: 1951
Format: Novel
Descriptor: Drugs as mind-expanders
Annotation: The Earth has been invaded by slug-like parasitic beings
that attach themselves to men's backs and dominate their
minds and bodies. The protagonists, Sam Nivin and Mary, are members
of a secret security agencyfighting the invaders. In the middle of
the struggle they decide to get married; but because they can only spare
24 hours for their honeymoon, they inject themselves with tempus, a
drug analogous to speed, which stretches subjective time for them so
that they feel they are experiencing a month-long honeymoon.
Author: Smith, George O.
Title: Hellflower
Publisher: Abelard Press, New York
Pages: 264 pp.
Date: 1953
Format: Novel
Descriptor: Drugs as sensation-enhancers
Annotation: On Ganymede, moon of Jupiter, grows the gardenia-like
plant from which hellflower, also known as love lotus,
is extracted—a narcotic which heightens sensations and other sensory
stimuli and creates psychological addiction through enhancement of
pleasure—with women the chief victims. Story concerns the traffic in
this and related drugs and the attempts of a government agent of the
future to intercept it.
Author: Devaux, Pierre and Viot, H. G.
Title: The stolen minute
Journal: Science Fiction Plus, Vol. 1, Nos. 4 and 5, 44-61,
42-62
Publisher: Gernsback Publications, Inc., New York
Date: June and August 1953
Format: Novel
Descriptor: Drugs as mind-expanders
Annotation: A French molecular physicist develops a drug known as
hexostyromolybdenum, HSM, which has the property of
vastly increasing the human metabolism. Motion, body speed, the rate
of living, and other functions are accelerated 100,000 times. Protagonists
make use of HSM to achieve desired political goals.
Author: Phillips, Rog (Pseud. for Roger Philip Graham)
Title: The yellow pill
Journal: Astounding. Science Fiction,Vol. 62, No. 2, 51-61
Publisher: Street & Smith Publications, New York
Date: October 1958
Format: Short story
Descriptor: Drugs as reality- testers
Annotation: Psychiatrist encounters a patient who has committed
murder and who has the delusion that he was on board
a spaceship, defending himself against lizard-men from Venus, at the
time of the killing. Patient totally denies the reality of actual world,
and tells psychiatrist to take a yellow pill that will awaken him to the
true reality of the spaceship-world. Psychiatrist is amused by concept
of a yellow pill-that can bring one out of a delusion; but then he
finds a bottle of yellow pills in his locker and the story becomes an
exploration of ambiguous levels of reality, with the pills serving as
conduits between one "real" world and the other.
Author: Purdom, Tom
Title: Greenplace
Journal: Fantasy and Science Fiction, Vol. 27, No. 5, 5-16
Publisher: Mercury Press , New York
Date: November 1964
Format: Short story
Descriptor: Drugs as intelligence enhancers
Annotation: Protagonist is a psychologist doing political field-testing
on behalf of a Congressman running for re-election c.1980. As he prepares to enter a suburban district controlled by his
candidate's powerful opponent, he doses himself with MST, a newly
invented psychic energizer that "multiplied the powers of observation
and the rate and quality of thought by a factor somewhere between
three and seven." Under the influence of MST he is able to detect the frightening psychological techniques by which the suburb is held in
control.
Author : McCombs, Larry and White, Ted
Title: The peacock king
Journal : Fantasy and Science Fiction, Vol. 29, No. 5, 23-36
Publisher: Mercury Press, New York
Date: November 1965
Format: Short story
Descriptor: Drugs as mind- expanders
Annotation: The United States is planning its first expedition into
interstellar space, using a radical space-drive that
permits faster-than-light travel. Preliminary experiments have shown
that a faster-than-light trip will have grave psychological impact on
the crew, and therefore LSD is used as part of the training discipline
for the crew (a man and a woman). Through acid experiences they
make themselves capable of handling the interstellar jump through
hyperspace.
Author: Dick, Philip, K.
Title: We can remember it for you wholesale
Journal: Fantasy and Science Fiction, Vol. 30, No. 4, 3-16
Publisher: Mercury Press, Inc., New York
Date: April 1966
Format: Short story
Descriptor: Drugs as mind-controllers
Annotation: A technique is developed by which, using a hypnotic
drug called narkidrine, false memories can be implanted
in a human brain. The memory-implant technique can be
used to provide the vicarious illusion of pleasurable experience, but
also—as the story unfolds—we see that it can be used for purposes
of political intrigue.
Author: Wilson, Colin
Title: The Mind Parasites
Publisher: Arkham House, Sauk City, Wisconsin
Pages : 222 pp.
Date: 1967
Format: Novel
Descriptor: Drugsasmind-expanders
Annotation: A research project involving heavy doses of mescaline
and LSD leads to perceptions revealing the existence of
invisible "mind parasites," alien invaders who have long controlled and
influenced human life. With the aid of the drug, experimenters unleash
mental powers with which to combat the invaders.
Author: Silverberg, Robert
Title: The World Inside
Publisher: Doubleday and Co., New York
Pages: 201 pp.
Date: 1971
Format: Novel
Descriptors: Drugs as mind-expanders, drugs as a means of
communication
Annotation: In world of 24th century, most of mankind lives in
thousand-story apartment buildings each of which has
a population of more than 800,000. Chapter three of the novel follows
the adventures of a musician who, after performing at a concert, drugs
himself with a multiplexer, a mind-expanding drug that temporarily
induces a telepathic contact simultaneously with all 800,000 residents
of his building, so that he perceives their lives and thoughts in one
vast intricate construct.
Author: Brunner, John
Title: The Stone That Never Came Down
Publisher: Doubleday and Co., New York
Pages : 206 pp.
Date: 1973
Format: Novel
Descriptor: Drugs as mind-expanders
Annotation: Scene is London, 1980's: a time of chaos with World
War III imminent. Chemists discover drug called VC—viral coefficient—which has the property of greatly intensifying sensory
perception and amplifying intelligence and memory. Drug has ability
to multiply in proper environment like living organism. When an unemployed
teacher who has had an experimental dose of VC donates blood
to cent ral bloodbank, he unwittingly spreads VC widely to the world at
large, causing an epidemic of sanity in which world leaders, now
greatly more intelligent, take steps to abolish warfare and establish
an ideally rational society.
Author: Dickson, Gordon R.
Title: The R-Master
Publisher: Lippincott, Philadelphia
Pages: 216 pp.
Date: 197 3
Format: Novel
Descriptor: Drugs as mind-expanders
Annotation: In the middle of the 21st century an intelligence-enhancing
drug called Reninase-47 has come into wide use. Though
normally it simply stimulates the thought process, R-47 occasionallv
does massive damage to the mind, and in a few cases creates a supergenius, an R-master. Protagonist's brother takes R-47 and suffers brain damage. In order to help him, protagonist also takes the drug
and unexpedtedly emerges from treatment as an R-master, a member
of an extraordinary elite group, and from another R-master he learns
of the need for a vast reorganization of governmental policies. He
becomes a revolutionary leader and works toward a transformation of
society.
Author: Spinrad, Norman
Title: The weed of time
Journal: Vertex, Vol. 1, No. 3
Publisher: Mankind Publishing Co. , Los Angeles
Pages: 58, 92-93
Date: 1973
Format: Short story
Descriptor: Drugs as mind-expanders
Annotation: An exploratory mission to the fifth planet of the star Tau
Ceti in 2048 discovers a plant that is given the name of
Tempis ceti, seeds and leaves of which have a psychedelic property:
they destroy the linear perception of time and enable the subject to view
all moments along his life span simultaneously. Seeds of the plant prove
to be fertile on Earth and the drug comes into common use. Protagonist
is a time-drug user whose simultaneous perception of his 110-year lifespan
sends him to a mental hospital.
Tourmal from Murray Leinster's Med Service Series. The animal has a special ability: if exposed to any disease (known or unknown), it will produce antibodies in quantity against it in about thirty seconds flat. The antibodies can be used to make a serum to protect against the diseease. Tourmals are used by the Med Service when they encounter planetary pandemics.
Anti-Acceleration Drugs
These are hypothetical drugs that help astronauts cope with high spacecraft acceleration or walking around on a heavy gravity planet. Keep in mind that if one has been in freefall for eight months on a Terra-Mars Hohmann trajectory, the one-third g of Mars will count as "heavy gravity" for your atrophied muscles.
In Poul Anderson's THE STAR FOX and in George O. Smith's VENUS EQUILATERAL series the drug Gravanol helps prevent damage if one is exposed to prolonged periods on a planet with more than 1.0 g of gravity, or multi-gravity acceleration on a spacecraft.
In The Expanse spacecraft pilots who need to function at accelerations higher than 1.0 g will go on "the juice". A set of auto-injectors built into the acceleration couch will pivot to the pilot's carotid arteries.
THE JUICE
The metal bars clamp on your neck and injects the juice into your jugular veins
"Alex, how long?" Holden asked for the third time in ten minutes.
"We're over an hour out. Want to go on the juice?" Alex said.
Going on the juice was pilot-speak for a high-g burn that would knock an unmedicated human unconscious. The juice was the cocktail of drugs the pilot's chair would inject into him to keep him conscious, alert, and hopefully stroke-free when his body weighed five hundred kilos. Holden had used the juice on multiple occasions in the navy, and coming down afterward was unpleasant.
"Not unless we have to," he said.
(ed note: if the apparent body weight is 500 kg, I figure the acceleration is on the order of seven gees)
Q: What is in the juice they take on the Roxinante (sic), and what is it doing?
DANIEL ABRAHAM: What it's doing is controlling blood pressure and the elasticity of blood vessels to try to keep you from stroking out. That's the big thing it's doing. The hardest thing about long, sustained high-G burns is that humans aren't used to them. So, it's something that will make sure that your blood pressure stays high enough so that you're getting blood all the way to your brain and that you're remaining elastic enough that you don't just pop like a balloon.
(ed note: there is also a second form of the juice that includes a sedative. This puts you to sleep for either hibernation or to knock you out for the duration of the burn. The first type of juice includes a stimulant to keep you from blacking out.
The writers of the TV version of The Expanse forgot to include the juice, but actor Cas Anvar thought the concept was cool and got it added in.)
From LEVIATHAN WAKES from The Expanse by "James S.A. Corey" 2011.
Combat Drugs
penciled by Jack Kirby inked by Frank Giacoia
Combat drugs are used to make soldiers more effective.
In the Traveller RPG, Combat drug increases a soldier's endurance and strength, but does cause medical damage to the user.
In SOLDIERS RUNNING by Brian Aldiss, both hostile nations are experimenting with drugs to increase the ability of their soldiers. The latest one is Fast-Plus, a sort of a hyperactivity inducing drug.
In The Tar-Aiym Krang by Alan Dean Foster, starship combat pilots use Heightened-Instinct-Perception drugs to become ultra deadly fighters.
FAST-PLUS
To wage war in its present form would not have been possible
without drugs. “ This is where you and your men come in. Colonel. Our
laboratories, bless ’em, have just turned up with a new wonder
drug called Fast-Plus. As far as I can understand, it’s a
development of the old pep pills. Unfortunately it’s still
rather in the experimental stage, but desperate situations call
fordesperate remedies …” A high-ranking medical man entered. In a pouch strapped
to his belt he carried the supply of Fast-Plus. This he would
administer when they reached the enemy forest ; now, he had
a preparatory tranquilizer for them which would render the
Fast-Plus more effective later. He administered this tranquilizer
to them orally just before they took off. The medico came round with the Fast-Plus, which was made
into boomerang-shaped capsules that fitted against the bottom
teeth under the tongue.
“ Don’t bite on them until the colonel gives the word,” he
said. “ And remember, don’t worry about yourselves. Just
get back to your plane and we’ll take care of the after effects.”
“ We’ll split into our five groups now,” the colonel said.
“ One and two to my left, four and five to my right. Seventy
seconds from now I’ll blow my whistle; crunch your pills then
and be off. Good luck. Move.” Twenty men moved. Four stayed with the colonel. Ignoring
the racket in the clearing, he watched the smallest hand on his
chronometer, whistle in his left fist. As he had hoped, the
noise had died as he blew his blast. He crunched his capsule
and rose, the four men beside him.
As they entered the forest, the drug took effect. A slight
dizziness seized the colonel, a singing started in his ears.
Against this minor irritation, a vast comfort swept through his
limbs. He began to breathe more rapidly, and then to think and
move more rapidly. His whole metabolism was accelerating. He had acted fast, hardly realising he was firing. The guns
they carried had special light-touch trigger actions to respond
to their new tempo. A burst of firing answered his shot, but it fell behind them.
They were moving faster, already breaking records. They passed caravans,
camouflaged vehicles, tanks, tents, some containing sleeping
men. All these they skirted. Anything moving they shot. A
fifty percent acceleration of perception and motion turned
them into supermen. They covered the first mile in five minutes, the second in
under four. Occasionally the colonel glanced at his wrist
compass, but a mystic sense seemed to keep him on course. When an unexpected burst of firing from a flank killed one
of the group, the other four raced on without pause. It was as
if they could never stop running. The second mile was easy, and most of the third. The machine gun posts opened up. Missing four phantoms’
they kept up their chatter in preparation for a main body of
men who never arrived. The phantoms plunged on, tormented
most by the noise, which bit like acid into their eardrums.
Several of the enemy were in the room. The firing nearby
had alarmed them. One spoke into a phone, while except for
one other the rest stared out of the windows anxiously. The
one other sat at the firing console. He saw the colonel first. Astonishment and fear came onto his face, slackening the
muscles there, dropping his mouth open. He slid round in his
seat, lifting his hand at the same time to reach out for the
press buttons. To the colonel, he appeared to be moving in
ultra-slow-motion, just as in ultra-slow-motion the other
occupants of the room were turning to face their enemy. Emitting a high squeal like a bat’s, the colonel twitched his
right index finger slightly. He saw the bullet speed home to its
mark. Raising hands to his chest, the push button man
toppled off his stool and fell beside the console.
They had four miles to go this way. After the first mile, the
maximum effect of the drug began to wear off. The colonel
was aware that the abnormal clarity of his brain was changing
into deadness. He ran on. At the end of the third mile, one of the colonel’s two men
collapsed without warning. His face was black and he hit the
ground with the sound of a felled tree, utterly burnt out. The
others never paused. The colonel and his fellow reached the rendezvous. They
lay twitching in a ditch until the plane came for them. By then
there were twelve twitching men to carry away, all that was left
of the original party. Two medical orderlies hustled them
rapidly into bunks, sinking needles into their arms to stop
their twitching.
This was Sgt. Taylor’s dream, and it woke him crying in his
hospital bed. Sgt. Taylor nodded vaguely, seeing the man’s lips move.
Well, they had said there might be after-effects. Perhaps
even now someone was inventing a drug to grow you new
eardrums … Heck, they should be able to think up some really bizarre
missions for a stone deaf man …
(ed note: The Humanx empire is a merger of the Human race and the Thranx insectoid race, who find that they perfectly complement each other like symbiont. Ensign Bran Tse-Mallory and his ship brother Truzenzuzex are combat stingship pilots in the Commonwealth space navy. They are in a task force that is standing on the sidelines as an atrocity is unfolding right before their eyes. The militant AAnn Empire is about to annex the Ornithorphe planet by invading and shooting anything that moves. The task force Major Gonzalez is a mealy-mouthed little coward who thinks this is not a Commonwealth problem. Brian and Truzenzuzex disagree.)
From above and behind him. Bran heard the voice of his young ship-brother. The insect’s deep blue-green chiton was rendered even more resplendent by the silver battle harness that enclosed its cylindrical body. ‘That,’ said Truzenzuzex in cool, even tones, ‘was just possibly the most nauseating bit of rhetorical doggerel it has ever been my misfortune to overhear.’ Bran agreed. He was finding it more and more difficult to restrain himself. Even without the heightened-instinct-perception drugs, the killing urge was beginning to steal warmly over turn. It had the powerful push of righteous indignation behind it.
Isn’t it possible that maybe the locals …?’ ‘… haven’t got a chance,’ finished Truzenzuzex. ‘They’re outnumbered and outgunned, and not a regular armed force among them in the first place. As the AAnn doubtlessly surmised well in advance. I doubt ‘f their ships even have doublekay drives. Theirs is only a colony and they wouldn’t have need of many. I can’t see dear sweet Gonzalez risking a chance to help a bunch of aliens, especially non-Commonwealth. He’s far too fond of his scotch and imported Terran cigars, Besides, to undertake such an action would require at least a modicum of imagination, a commodity in which our commander is sadly deficient. Look. It’s starting already.’ Bran glanced up above the communications equipment to the huge battle screen. Out in the void a number of ships represented only by ghostly dots were manoeuvring across thousands of kilometres for position in a battle which would prove notable only for its brevity. Somehow the locals had mustered six space-worthy ships. He’d bet a year’s credit not one of them was a regular warship. Police launches, most likely. Opposite, the well-drilled, superbly disciplined AAnn force was to lining one of its characteristic tetrahedrons. Fifteen or so attack ships, a couple of destroyers, and two bloated pips that in a normal battle situation he would have interpreted as dreadnoughts. The finer instruments on the big board told the true story: same mass, small gravity wells. Troop carriers, nursing dozens of small, heavily screened troop shuttles. He slammed a fist down on the duralloy board, scraping the skin on the soft underside of his wrist. There were ten stingers and a cruiser in the Humanx force … more than a match for the AAnn, even without the dubious ‘help’ of the locals. But he knew even before the pathetic debate of a few moments ago that Major Gonzalez would never stir from his wood-panelled cabin on the Altair to intervene in any conflict where Humanx interests weren’t directly threatened. He paused at a sudden thought. Of course, if a confrontation could be forced to the point that such a threat occurred … still no certain guarantee … definite court-martial … dismissal from the Corps … 300,000 sentient beings … processing camps… He suddenly wasn’t so sure that he wanted to make captain after all. Still, he’d need the concurrence of… ‘Bran, our drive appears to lie malfunctioning.’ ‘Wha? I don’t…’ ‘Yes, there is no question about it. We appear to be drifting unavoidably into the area of incipient combat. At top speed, no less. A most unusual awkwardness, wouldn’t you agree?’ ‘Oh. Oh, yes.’ A pseudo-smile sharp as a scimitar cut his face. “I can see that we’re helpless to prevent it. God damn unfortunate situation. Naturally we’ll have to make emergency preparations to defend ourselves. I don’t think the AAnn computers will be overly discerning about ships which float into their target area.’ ‘Correct. I was just about to commence my own injections.’ ‘Myself also.’ He snuggled back into the reaction seat, felt the field that enabled them to manoeuvre at high speed and still live take hold gently. ‘Best hurry about it.’ He followed accepted procedure and did his best to ignore the barely perceptible pressures of the needles as they slipped efficiently into the veins on his legs. The special drugs that heightened his perceptions and released the artificial inhibitions his mind raised to constrain the killer instinct immediately began to take effect, A beautiful rose-tinted glow of freedom slipped over his thoughts. This was proper. This was right. This was what he’d been created for. Above and behind him he knew that Truzenzuzex was undergoing a similar treatment, with different drugs. They would stimulate his natural ability to make split-second decisions and logical evaluations without regard to such distractions as Hive rulings and elaborate moral considerations. Shortly after the Amalgamation, when human and thranx scientists were discovering one surprising thing after another about each other, thranx psychologists unearthed what some humans had long suspected. The mind of Homo sapiens was in a perpetual state of uneasy balance between total emotionalism and computer-like control. When the vestiges of the latter, both natural and artificial, were removed, man reverted to a kind of control-led animalism. He became the universe’s most astute and efficient killing machine. If the reverse was induced he turned into a vegetable. No use had been found for that state, but for the former … It was kept fairly quiet. After a number of gruesome but honest demonstrations put on by the thranx and their human aides, mankind acknowledged the truth of the discovery, with not a small sigh of relief. But they didn’t like to be reminded of it. For their part human psychologists brought into clearer light the marvelous thranx ability to make rapid and correct decisions with an utter lack of emotional distraction and a high level of practicality. Only, the thranx didn’t think it so marvellous. Their Hive rulings and complicated systems of ethics had long kept that very same ability tied down in the same ways humanity had its killer desires. The end result of all the research and experimentation was this: in combination with a ballistics computer to select and gauge targets, a thranx-human-machine triumvirate was an unbeatable combination in space warfare. Thranx acted as a check on human and human as a goad to thranx. It was efficient and ruthless. Human notions of a ‘gentleman’s’ war disappeared forever. Only the AAnn had ever dared to challenge the system more than once, and they were tough enough and smart enough to do it sporadically and only when they felt the odds to be highly in their favour. It was fortunate that thranx and human proved even more compatible than the designers of the system had dared hope — because the nature of the drug-machine tie-up resulted in a merging of the two minds on a conscious level, it was as if the two halves of a brain were to fight out a decision between themselves, with the compromise then being paused on to the spinal cord and the rest of the body for actual implementation, Some stingship pilots likened it more closely to two twins in the womb. It was that intimate a relationship. Only in that way would the resultant fighting machine operate at 100 per cent effectiveness. A man’s partner was his ship-brother. Few stinger operators stayed married long, except those who were able to find highly understanding wives. The tingling mist flowed over his eyes, dimming and yet enhancing his vision. The tiniest things became obvious to his perception. Specks of dust in the cabin atmosphere became clear as boulders. His eyes fastened on the white diamonds on the battle screen with all the concentration of a starving cobra. All stinger pilots admitted to a slight but comforting sense of euphoria when under battle drugs. Bran was experiencing it now. For public relations purposes the enforcement posters insisted it was a beneficial byproduct of the HIP drugs. The pilots knew it for what it was; the natural excitement that overtakes most completely uninhibited humans as they anticipate the thrill of the kill. His feelings whirled within, but his thoughts stayed focused. His hand drifted down to the firing studs. The calm voice of Truzenzuzex insinuated itself maddeningly in his mind. No, it was already in his mind. ‘Hold. Not yet,’ Pause. ‘Probability.’ He tried angrily to force the thought out and away. It wouldn’t go. It was too much like trying to cut away part of one’s own ego. His hand stayed off the firing stud as the cream-coloured dot grew maddeningly large in the screen. Again the calm, infuriating voice. ‘Changing course ten degrees minus y, plus x two degrees achieve optimum intercept tangent.’ Bran knew they were going to die, but in his detached haze of consciousness it seemed an item of only peripheral importance. The problem at hand and the sole reason for existence was to kill as many of them as possible. That their own selves would also be destroyed was a certainty, given the numbers arrayed against them, but they might at least blunt the effect of the AAnn invasion. A tiny portion of him offered thanks for Truzenzuzex’s quiet presence. He’d once seen films of a force of stingships in action with only human operators. It had resembled very much a tridee pix he’d seen on Terra showing sharks in a feeding frenzy. The moment notified him of itself. ‘Firing one!’ There were no conflicting suggestion from the insectoid half of his mind. He felt the gentle lurch of his body field as the ship immediately executed an intricate, alloy-tearing manoeuvre that would confuse any return fire and at the same time allow them to take the remaining two enemy vessels between them. Without the field he would have been jelled. The disappearance of a gravity well from the screen told him that the SCCAM projectile had taken the AAnn ship, piercing its defences. A violent explosion flared silently in space. A SCCAM was incapable of a ‘near-miss.’ The SCCAM system itself was a modification of the doublekay drive that powered the ships of most space-going races (SCCAM stands for Severely Concentrated and Catastrophic Accelerated Motion). When human and thranx met it was found that the human version was more powerful and efficient than the thranx posigravity drive. It also possessed a higher power-conservation ratio, which made it more reasonable to operate. Working with their human counterparts after the Amalgamation, thranx scientists soon developed a number of improvements in the already remarkable system. This modified propulsive drive was immediately installed in all Humanx ships, and other races to order the components which would enable them to make their own modifications. A wholly thranx innovation, however, had been the adaption of the gravity drive as a weapon of irresistible power. The SCCAM projectiles were in actuality thermonuclear devices mounted on small ship drives, with the exception that all their parts other than those requiring melting points over 2400 degrees were made of alloyed osmium. Using the launching vessel’s own gravity well as the initial propelling force, the projectile would be dispatched toward a target. At a predetermined sate distance from the ship, the shell’s own drive would kick in. Instantly the drive would go into deliberate overload. Impossible to dodge, the overloaded field would be attracted to the nearest large gravity well in this case, the drive system of an enemy ship. Coupled with the uncontrolled energy of a fusion reaction, the two intersecting drive fields would irrevocably eliminate any trace of the target. And it would be useless for an enemy vessel to try to escape by turning off its own field, for while it might survive impact with the small projectile field, the ship had not yet been constructed that could take the force of a fusion explosion unscreened. And as the defensive screens were powered by the posigravity drives … He felt the ship lurch again, not as violently this time. Another target swung into effective range. He fired again. Truzenzuzex had offered a level-four objection and Bran had countered with a level-two objective veto. The computer agreed with Bran and released the shell. Both halves of the ship-mind had been partially correct. The result was another hit … but just barely. Bran had just gotten off a third shot — a miss — when a violent concussion rocked the stinger. Even in his projective field he was jerked violently forward. The lights flickered, dimmed, and went off, to be replaced a moment later by the eerie blue of the emergency system. With the cessation of the ship’s capacity for battle the HIP antidotes had automatically been shot into his system. Thank Limbo the automedics were still intact! He felt the killing urge flow out of him, heavily, to be replaced by the dull aftertaste and temporary lethargy that inevitably followed battle action. He hadn’t realized, in the comfort of HIPnosis, how badly the little vessel had been damaged. Torn sheeting and wavering filaments floated everywhere, indicating a loss of shipboard gravity. But the pod had remained intact and he could breathe without his hoses.
(ed note: When they look into the scanners they discover that the other stingship pilots have joined them and are proceeding to kick the living snot out of the AAnn ships, while Major Gonzalez sputters ineffectually.
In the court-martial Bran and Truzenzuzex are dismissed from the Corps, but first they are both awarded the Order of Merit with one star cluster. And presented with scrolls on which the citizens of the planets had inscribed their names and thanks.
Major Gonzalez was give a desk job in an obscure system populated by semi-intelligent amphibians.)
In response to the verbal from the autopilot, Dieter Ulans flipped his datavisor in front of his eyes and prepared to take direct command of the massive ring of lasers and reaction engines that was Hercules. He hit the juicer button and felt the rush as the drugs began to wash into his veins. "Com'mon jockey juice!" he whispered. The tiny green symbols on the datavisor began to zip past his eyes at an increasing speed.
His subconscious easily absorbed and processed the information even as his conscious mind took in the blue numbers and symbols on the main screen that showed the gross situation as Hercules and five other ships of the Martian battlefleet began their final approach to Vesta Main Station. The ship thrummed as the main three o'clock engine cut in and changed vector in response to a movement of Dieter Ulan's right ring finger.
A second green line began streaming across the datavisor as Ulans took control of the main laser fire control systems. Every time he blinked, the little green symbols paused. Every time he squinted his eyelids, a bright blue bullseye magically appeared where he looked on the main screen. Just tap your foot when your buddy shows, he thought, and you'll make him a star.
From the introduction to the wargame BATTLEFLEET MARS by Redmond Simonsen
If you drank too much alcohol the night before, waking up is not going to be pretty. Currently there are no 100% effective hangover remedies but hopefully future medical science will invent a cure.
Also in science fiction are drugs that prevent one from becoming inebriated no matter how much alcohol is consumed, such as the "soberpills" from Poul Anderson's STAR WAYS. While no fun at all at a party, such drugs are useful when one wants to keep a clear head while your target or mark is trying to drink you under the table.
ALTAN HERB
The following morning, Drake received a call from Commodore-Lord Bardak. “Good morning, sir,” Drake said when the Sandarian commander’s features solidified in the workscreen in his cabin.
“And to you, Fleet Captain Drake,” Bardak boomed. “How’s your head?”
“About as you would expect after last night’s round of toasts.”
Bardak nodded. “I feel as though someone is trying to dig his way out of my skull.”
“I am in somewhat better shape,” Drake replied. “There is an Altan herb that goes a considerable way toward alleviating the worst symptoms of a hangover. It doesn’t make you feel good, mind you; but, at least you aren’t miserable.”
“Such a wonder would be one of the first things we would want to import when interstellar trade resumes.”
“We have a concoction. Vitamins. Tonic. Other stuff. Works every time. Would you care for some?” “Captain, I would kill for a glass of that. Or two glasses. Please?” Owensford grinned. “This way.” He led Lysander to a small bar at the far end of the officers’ mess, and ushered him to a table. Billings, two Night Befores, please.” “Sir.” The bartender was an old man, but he carried himself like a soldier. His left hand was a prosthetic adapted to bartending. He grinned and set two tall glasses on the table, went back, and brought a pitcher of water. “You sip it,” Owensford said. “Then down at least two glasses of water. Works like a charm.” Lysander sipped, and grimaced. “I didn’t say it tasted good,” Owensford said. “This late, we’re lucky to get anything at all. Anyway, you look a lot more chipper than you did half an hour ago.” “I’m going to take the formula for that vitamin gunk back to Sparta. We’ll make it a government monopoly and after five years we’ll be able to abolish taxes.” He clinked his coffee mug against hers.
From PRINCE OF MERCENARIES by Jerry Pournelle (1989)
ALCODOTE-VITAMIN PILLS
“Get a little rest, for a couple of hours. Then draw some
alcodote-vitamin pills from the medic. As soon as things are
secured, there'll be parties all over the ship, and we'll be
expected to look in on every one of them, have a drink, and say
‘Well done, boys!’”
From SPACE VIKING by H. Beam Piper (1963)
SOBERING-EFFECT
"I wish I didn' have to do this—" Basurero shuddered and took from the shelf a jar labeled SOBERING-EFFECT, THE ORIGINAL INSTANT CURE FOR INEBRIATION—NOT TO BE TAKEN WITHOUT A DOCTOR'S PRESCRIPTION AND A LIFE INSURANCE POLICY. He extracted a polka-dotted, walnut-sized pill, looked at it, shuddered, then swallowed it with a painful gulp. His entire body instantly began to vibrate, and he closed his eyes as something went gmmmmph deep inside him and a thin trickle of smoke came from his ears. When he opened his eyes again they were bright red but sober. "What is it?" he asked hoarsely.
From BILL THE GALACTIC HERO by Harry Harrison (1965)
KILLALC PILLS
As we walked to the officers' club I was in no mood for communication, which Otrov probably blamed on my recent demotion. What to do? Drink seemed to be in order, it wasn't noon yet, and it would be wisest to wait until evening to crack out of the base. Face the problems as they arose. Right now I was in a perfect position to imbibe drink with my new peer group and gather information at the same time. Which, after all, was the reason that I was here in the first place. Before leaving I had slipped a tube of killalc pills into my pocket. One of these every two hours would produce a massive heartburn, but would also grab onto and neutralize most of the alcohol as soon as it hit the stomach. I would drink deep and listen. And stay sober. As we walked through the garish doorway of the club I slipped one out and swallowed it.
At that moment the duty siren sounded. The uproar redoubled. Military Police came pouring into
the mess, pushing and kicking the drunks onto their feet and
marching them out of the door. Just outside, a tube truck was waiting. The Special Wing
staggered or was pushed into it. When all were accounted for,
the doors closed and the tube moved off, snoring into the tunnel
on an upward gradient. It stopped again at Medical Bay, where orderlies with
alcoholometers awaited them. Anyone who flipped the needle
was instantly given an anti-toxic drug. The colonel, for all
that he had drunk little, had to submit to an injection. The
alcohol in his blood was neutralised almost at once. Within
five minutes, everyone in the room was stone cold sober again.
To wage war in its present form would not have been possible
without drugs.
These are drugs that put a person into a months-long coma (like a hibernating bear) or actually allow them to be frozen as a static block of ice (suspended animation) to drastically reduce consumption of life support air and food. Or to stabilize a crewmember who is seriously ill or injured when the ship cannot return to Terra for another two years.
In the RPG TravellerFast drug puts the user into hibernation for 60 days during which they require only 1 day's worth of oxygen and food.
In Arthur C. Clarke's CHILDHOOD'S END the drug Narcosamine is used to induce hibernation, reducing consumables required for prolonged spaceflight.
In Jack Williamson's LIFEBURST the drug Metabrake is used to induce hibernation to assist surviving space disasters. Survivors need to recover in sick-bay, while counteractants are used to flush the metabrake out of the patient's system. In his earlier novel TRAPPED IN SPACE he calls it a "deep-sleep shot", and it is calibrated to wear off at a given point in time. When the shot wears off, medical attention is required immediately.
In the real world, spaceflight researchers are studying how to induce hibernation. Methods being studied include Therapeutic Hypothermia (temperature-based hibernation), Chemical/Drug-based (hydrogen sulfide or activating adenosine receptors), and Brain Synaptic-based.
NARCOSAMINE
He took out the little syringe, already loaded with the carefully prepared solution. Narcosamine had been discovered during research into animal hibernation: it was not true to say — as was popularly believed — that it produced suspended animation. All it caused was a great slowing-down of the vital processes, though metabolism still continued at a reduced level. It was as if one had banked up the fires of life, so that they smoldered underground. But when, after weeks or months, the effect of the drug wore off, they would burst out again and the sleeper would revive. Narcosamine was perfectly safe. Nature had used it for a million years to protect many of her children from the foodless winter.
From CHILDHOODS END by Sir Arthur C. Clarke
METABRAKE
Metabrake. A drug regimen used to induce human hibernation
during space emergencies. It lowers body temperature and slows
all metabolic processes, reducing needs for oxygen, water, and
food. Side effects varied, sometimes fatal. Survival depends on
age, health, tissue mass, competent medical care, and duration of
coma. In exceptional cases, revival has been successful after
almost a year.
“Buzz isn’t sure what he can do,” she said. “But
it’s going to hurt, when he explores the wound. Buzz
says we ought to give him something to put him to
sleep, but there’s nothing in the aid kit.” “I can stand some pain,” Ty whispered. “Wait!” Jeff broke in. “Can’t we use a deep-sleep
shot?” Buzz whistled at Lupe. “Buzz has heard about deep sleep,” she said. “He
wants to know more about it.” “It was invented to help men live through accidents in space,” Jeff said. “It slows life to the very
point of death. In deep sleep, you need no food or
warmth or even air. You can wake up from it, if you
get care in time.” Buzz whistled quickly, and Lupe said, “He wants
to see the drug.” Jeff showed Buzz a sealed green package in the
medical kit, then broke the seal to pull out a small
needle and a timer. “The needle is marked in hours,” Jeff told him.
“You set the slide for the weight of the patient. The
smallest shot gives about three hours of deep sleep.
The whole needle gives a thousand hours. That’s the
limit. The timer tells when care has to be started.”
Drugs that amplify intelligence (temporarily or permanently) are technically called Nootropics (aka smart drugs, memory enhancers, neuro enhancers, cognitive enhancers, and intelligence enhancers).
R-47 from Gordon Dickson's THE R-MASTER
VC (viral coefficient) from John Brunner's THE STONE THAT NEVER CAME DOWN
Hormone K Treatment from Ted Chiang's UNDERSTAND
Methuen Treatment from L. Sprague de Camp's THE EXALTED
IQ Boosters from Charles Pellegrino and George Zebrowski THE KILLING STAR
IQ BOOSTERS
THE IQ BOOSTERS WORKED SWIFTLY, SURGING UP through the arteries in her neck, seeking the outer layers of the neocortex. Manufactured from algae that had been genetically tricked into producing human enzymes, one set of boosters more than tripled the rate at which nerves recharged and fired, while other substances increased the growth of new nerve connections and modulated energy efficiency. It was the increase in firing frequency that had the first and most profound effect. After only two days on the boost, Tarn and her crew were connecting disparate and seemingly unrelated facts faster than they had ever before in their entire lives, possibly faster than any human beings since the beginning of time.
One side effect of her newly acquired abilities was that she could now clearly see the flicker of her liquid crystal display pad, which usually cycled too quickly for the human eye to register. Watching the pad (especially in the 3-D mode) became an activity guaranteed to trigger migraine, and she worried that there might be other unanticipated effects. Yet they were all being forced to think faster, to redesign their own brain chemistries, and, whenever necessary, to experiment upon themselves. They had no choice.
From THE KILLING STAR by Charles Pellegrino and George Zebrowski
Interrogation Drug
These are super-duper versions of "truth serum". The difference is that the science fictional versions actually work.
Fast-Penta from Lois McMaster Bujold's MILES VORKOSIGAN series
"Moment of Truth" from James Schmitz's LION LOOSE
Related are the Focus Drugs from The Expanse. They are not used on the person being questioned, instead they are used by the interrogator. It turns them into a super-duper human lie detector. They can spot fractional second changes of expression and other tells exhibited by the person being questioned.
When Expanse co-author Daniel Abraham was asked about focus drugs he said: "Well, it’s a nootropic drug. We don’t specify exactly what it is, but it’s job is to increase focus, to cut away the distractions and to allow people to hyper-focus on whatever it is that they’re doing Um, it’s not unlike what we do with Ritalin."
Medical Drugs
These are drugs used by doctors, nurses, and emergency workers to heal the sick and injured.
In the RPG Traveller, Panacea drug augments healing and Medical Slow drug puts the user into a coma for one day during which they experience a month's worth of healing.
In the RPG Space Opera, a person at death's door can be administered the drug Thanokalamine. This will arrest decay of all body tissue (including the brain and nervous system) long enough to get them to a hospital with Death Revival capability. Shrewd people in dangerous lines of work wear PMS personal medisensor bracelets that monitor their body's vital signs, injecting thanokalamine at need. The comic Murphy's Rules asks the awkward question: how can the drug circulate through the body if the victim's heart has already stopped? A less drastic drug Quicktime Regen rapidly increases wound healing rates.
Star Trek had "tri-ox compound." It is a intravenous medicine used for rapidly oxygenating the blood cells of a living being. Useful if the patient had their space suit oxygen tanks run dry or are otherwise suffocating. As with so many other scifi concepts predicted by Star Trek, this one came true. Doctor McCoy saved Captain Kirk's life with this in The Tholian Web. He did it a second time by pretending to inject Kirk with Tri-ox in the guise of compensating athletic performance in the relatively low oxygen atmosphere of the planet Vulcan (but instead slipped Kirk a mickey). However tri-ox would have made Kirk's blood flush with oxygen. Which means Olympic coaches everywhere are desperately trying to get their hands on the real world version of the stuff to give their athletes an edge.
UNIVERSAL ANTIBIOTIC
(ed note: Burton has been infected with the deadly Andromeda Strain. He has a request.)
At that moment, Burton said over the intercom, "Listen. I want you to try something for me."
Stone flicked on the microphone. "What?"
"Kalocin," Burton said.
"No." Stone's reaction was immediate.
"Dammit, it's my life."
"No," Stone said.
Hall said, "Maybe we should try—"
"Absolutely not. We don't dare. Not even once."
Kalocin was perhaps the best-kept American secret of the last decade. Kalocin was a drug developed by Jensen Pharmaceuticals in the spring of 1965, an experimental chemical designated UJ44759W, or K-9 in the short abbreviation. It had been found as a result of routine screening tests employed by Jensen for all new compounds.
Like most pharmaceutical companies, Jensen tested all new drugs with a scatter approach, running the compounds through a standard battery of tests designed to pick up any significant biologic activity. These tests were run on laboratory animals— rats, dogs, and monkeys. There were twenty-four tests in all.
Jensen found something rather peculiar about K-9. It inhibited growth. An infant animal given the drug never attained full adult size.
This discovery prompted further tests, which produced even more intriguing results. The drug, Jensen learned, inhibited metaplasia, the shift of normal body cells to a new and bizarre form, a precursor to cancer. Jensen became excited, and put the drug through intensive programs of study.
By September 1965, there could be no doubt: Kalocin stopped cancer. Through an unknown mechanism, it inhibited the reproduction of the virus responsible for myelogenous leukemia. Animals taking the drug did not develop the disease, and animals already demonstrating the disease showed a marked regression as a result of the drug.
The excitement at Jensen could not be contained. It was soon recognized that the drug was a broad-spectrum antiviral agent. It killed the virus of polio, rabies, leukemia, and the common wart. And, oddly enough, Kalocin also killed bacteria.
And fungi. And parasites.
Somehow, the drug acted to destroy all organisms, built on a unicellular structure, or less. It had no effect on organ systems— groups of cells organized into larger units. The drug was perfectly selective in this respect.
In fact, Kalocin was the universal antibiotic. It killed everything, even the minor germs that caused the common cold. Naturally, there were side effects— the normal bacteria in the intestines were destroyed, so that all users of the drug experienced massive diarrhea— but that seemed a small price to pay for a cancer cure.
In December 1965, knowledge of the drug was privately circulated among government agencies and important health officials. And then for the first time, opposition to the drug arose. Many men, including Jeremy Stone, argued that the drug should be suppressed.
But the arguments for suppression seemed theoretical, and Jensen, sensing billions of dollars at hand, fought hard for a clinical test. Eventually the government, the HEW, the FDA, and others agreed with Jensen and sanctioned further clinical testing over the protests of Stone and others.
In February 1966, a pilot clinical trial was undertaken. It involved twenty patients with incurable cancer, and twenty normal volunteers from the Alabama state penitentiary. All forty subjects took the drug daily for one month. Results were as expected: normal subjects experienced unpleasant side effects, but nothing serious. Cancer patients showed striking remission of symptoms consistent with cure.
On March 1, 1966, the forty men were taken off the drug. Within six hours, they were all dead.
It was what Stone had predicted from the start. He had pointed out that mankind had, over centuries of exposure, developed a carefully regulated immunity to most organisms. On his skin, in the air, in his lungs, gut, and even bloodstream were hundreds of different viruses and bacteria. They were potentially deadly, but man had adapted to them over the years, and only a few could still cause disease. All this represented a carefully balanced state of affairs. If you introduced a new drug that killed all bacteria, you upset the balance and undid the evolutionary work of centuries. And you opened the way to superinfection, the problem of new organisms, bearing new diseases.
Stone was right: the forty volunteers each had died of obscure and horrible diseases no one had ever seen before. One man experienced swelling of his body, from head to foot, a hot, bloated swelling until he suffocated from pulmonary edema. Another man fell prey to an organism that ate away his stomach in a matter of hours. A third was hit by a virus that dissolved his brain to a jelly.
And so it went.
Jensen reluctantly took the drug out of further study. The government, sensing that Stone had somehow understood what was happening, agreed to his earlier proposals, and viciously suppressed all knowledge and experimentation with the drug Kalocin.
An intravenous infusion of oxygen-filled microparticles (the yellow sphere in this composite image) could carry the life-sustaining gas to red blood cells.
The stuff looks like foam. Which probably means the caliber of the needle required is terrifying
(ed note: technical term is apparently Intravenous Oxygen or Injectable Oxygen)
Boston, Mass. - Patients unable to breathe because of acute lung failure or an obstructed airway need another way to get oxygen to their blood—and fast—to avoid cardiac arrest and brain injury. A team led by researchers at Boston Children’s Hospital has designed tiny, gas-filled microparticles that can be injected directly into the bloodstream to quickly oxygenate the blood.
The microparticles consist of a single layer of lipids (fatty molecules) that surround a tiny pocket of oxygen gas, and are delivered in a liquid solution. In a cover article in the June 27 issue of Science Translational Medicine, John Kheir, MD, of theDepartment of Cardiology at Boston Children’s Hospital, and colleagues report that an infusion of these microparticles into animals with low blood oxygen levels restored blood oxygen saturation to near-normal levels, within seconds. When the trachea was completely blocked— a more dangerous “real world” scenario—the infusion kept the animals alive for 15 minutes without a single breath, and reduced the incidence of cardiac arrest and organ injury.
The microparticle solutions are portable and could stabilize patients in emergency situations, buying time for paramedics, emergency clinicians or intensive care clinicians to more safely place a breathing tube or perform other life-saving therapies, says Kheir.
“This is a short-term oxygen substitute—a way to safely inject oxygen gas to support patients during a critical few minutes,” he says. “Eventually, this could be stored in syringes on every code cart in a hospital, ambulance or transport helicopter to help stabilize patients who are having difficulty breathing.” The microparticles would likely only be administered for a short time, between 15 and 30 minutes, because they are carried in fluid that would overload the blood if used for longer periods, Kheir says.
Kheir also notes that the particles are different from blood substitutes, which carry oxygen but are not useful when the lungs are unable to oxygenate them. Instead, the microparticles are designed for situations in which the lungs are completely incapacitated.
Kheir began investigating the idea of injectable oxygen in 2006, after caring for a little girl who sustained a severe brain injury resulting from a severe pneumonia that caused bleeding into her lungs and severely low oxygen levels. Despite the team’s best efforts, she died before they could place her on a heart-lung machine. Frustrated by this, Kheir formed a team to search for another way to deliver oxygen.
“Some of the most convincing experiments were the early ones,” he says. “We drew each other’s blood, mixed it in a test tube with the microparticles, and watched blue blood turn immediately red, right before our eyes.”
Over the years, Kheir and his team have tested various concentrations and sizes of the microparticles to optimize their effectiveness and to make them safe for injection. “The effort was truly multidisciplinary,” says Kheir. “It took chemical engineers, particle scientists and medical doctors to get the mix just right.”
In the studies reported in the paper, they used a device called a sonicator, which uses high-intensity sound waves to mix the oxygen and lipids together. The process traps oxygen gas inside particles averaging 2 to 4 micrometers in size (not visible without a microscope). The resulting solution, with oxygen gas making up 70 percent of the volume, mixed efficiently with human blood.
“One of the keys to the success of the project was the ability to administer a concentrated amount of oxygen gas in a small amount of liquid,” Kheir says. “The suspension carries three to four times the oxygen content of our own red blood cells.”
Intravenous administration of oxygen gas was tried in the early 1900s, but these attempts failed to oxygenate the blood and often caused dangerous gas embolisms.
“We have engineered around this problem by packaging the gas into small, deformable particles,” Kheir explains. “They dramatically increase the surface area for gas exchange and are able to squeeze through capillaries where free gas would get stuck.”
Remember all drugs are poisons, and all poisons are drugs; the only difference is the dosage. For most poisons, there exists an antidote that will prevent the poison from killing the victim if it is administered in time. Some poisons have no antidote, e.g.,Aconitine. In less scientific eras con-artists did a brisk trade in bogus "universal antidotes" with kings, aristocracy, and other wealthy assasination targets. In more scientific eras this con might continue, only replacing the description "powered unicorn horn" with something like "nanotechnology."
Technically a "toxin" is a poison that is produce by a plant or animal in nature (instead of being brewed up in a chemical lab by an assasin). A "venom" is a toxin that an animal injects by a bite or sting. The old rule-of-thumb is: If you bite an animal and you die, the animal is poisonous. If the animal bites you and you die, the animal is venomous.
In David Brin's The Uplift War, the Gubru invaders have to deal with resistance from native partisans(guerrilla warfare, with uplifted gorillas). To deal with this, the Gubru use what is called "hostage gas" or "coercion gas". When they find a knot of guerrilla resistance in the jungle, they hose the place down with hostage gas and announce that the gas is poison that will kill in a few days. The gassed guerrilla have a choice of [a] turning themselves in at the POW camp and getting a shot of the antidote or [b] dying hideously.
In Frank Herbert's DUNE there is a remarkably nasty innovation called a Residual Poison.
With most poisons, a victim who is given the proper antidode will not die, and the poison will be flushed out of the body.
With a dreaded residual poison, the antidote will spare the life of the victim but the poison will remain in the body forever. The victim must receive a daily dose of the antidote for the rest of their lives to prevent death. This puts them at the mercy of the poisoner. Unless they follow all commands of the poisoner they will die when the antidote is withheld. The only way to be freed from being the poisoner's slave is to [a] discover the identity of the antidote and [b] secure a life-time supply of the stuff.
A really underhanded poisoner may dose their victim with both the residual poison and the antidote in secret, if they can plausibly prevent the victim from scanning their food with a Dune Poison Snooper . The victim will have no idea that their lifespan is now at the whim of the poisoner, until the most dramatic moment. All the poisoner has to do is to covertly ensure that the victim is regularly fed the antidode. The victim can use a poison snooper all they want. Since the antidote is not a poison, the snooper will return a null reading.
In this case, for a victim to be freed from being the poisoner's slave requres an additional step [c] discover that you were residual poisoned in the first place.
The poisoner who wants to secretly dose somebody with a residual poison has a monumental task. The Dune aristocracy is so ultra-paranoid about being poisoned that use of a poison snooper is obsessively done. This is because assasination by poison is so common in the Dune universe that they actually have separate words for poisons in the food and poisons in drinks.
Prolonged Lifespan Drug
Medicine holding back Death, by Julian Home Harris, 1959
On Fulton County Department of Health and Wellness
Yes, I know he is holding the wrong staff, should be Rod of Asclepius. Just roll with it, OK?
These drugs make one "immortal" in the sense of becoming partially or fully immune to dying from old age. You can still die from starvation, being blown out an airlock with no spacesuit, or being drilled between the eyes by a laser rifle.
Such drugs do NOT make one immortal in the sense of "invulnerability" or being remarkably difficult to kill with clubs, swords, or firearms (Wolverine-like levels of regeneration, resurrection from the dead like Count Dracula, that sort of thing).
Obviously the existence of such drugs will have a drastic affect on society. Since nobody wants to die such drugs will be fantasically expensive/valuable, and probably controlled substances if not flat-out illegal. Meaning there will be a huge black market and organized-crime operation.
In James Blish's CITIES IN FLIGHT series such drugs are called "Anti-Agathic". The term is derived from Greek agathos, “good,” presumably Mr. Blish confused this with thanatos, “death”. Unless he meant that such drugs destroy good.
Digestive of Gerald Kersh's "WHATEVER HAPPENED TO CORPORAL CUCKOO?"
Boosterspice from Larry Niven's "KNOWN SPACE" series
Antigerone in John Wyndham's TROUBLE WITH LICHEN
Stroon / Santaclara from Cordwainer Smith's INSTRUMENTALITY OF MANKIND series
The spice Melange from Frank Herbert's DUNE novels
In Robert Forward's FLIGHT OF THE DRAGONFLY aka ROCHEWORLD, the drug No-Die slows the aging process to one-fourth the normal rate. Unfortunately it temporarily lowers intelligence by roughly the same factor.
For the 42 year slower-than-light interstellar mission, the planners chose astronauts with higher than normal IQ. This was so No-Die only lowered their intelligence to that of a small child instead of to that of a newborn infant. The crew was looked after by the ship's computer, until the destination was reached. This allowed the crew to arrive and start exploring Alpha Centauri with an average biological age of 40 years instead of 72.
Most of the time, it looks like a pint of grayish fluid in a bag, a little saline, with a faint rainbow sheen. Intravenous tubing included. Responsible medical supervision not included.
But inject it into your veins — ah, then the magic happens. It splices, it lyses. It unwraps storage plasmids and writes then into your chromosomes, injects nanocytes into your cells, builds nanogenic artificial lymph glands to keep your system stocked with roaming nanocytes, and even tidies up your gross morphology a bit, especially if you were already old. (While you develop a high fever and a really nasty set of aches and pains for a week or two — the more so the more gross work it has to do. Don’t even ask what your excreta look like.)
These are drugs that bestow or amplyfy mystical magical psionic powers.
The mutagen ephemerol from the movie SCANNERS causes pregnant women to give birth to children with psionic powers.
In the RPG Traveller, Psi-Booster drug temporarily increases an already psionic person's power a little, Psi-Double drug temporarily increases a psi's power a lot, and Psi-Special drug hourly increases a psi's power up to the maximum, then drops back to normal.
The spice Melange from Frank Herbert's DUNE novels sometimes grants the psionic ability of seeing the future.
And in many science fiction novels there are drugs that suppress psionic powers, used by the authorities to control psionic people. Otherwise the cops can't keep teleporters from escaping their jail cells. In Babylon 5 all telepaths have to either join the Psi Corps and be subjected to their discipline, or a Psi Cop shows up once a week to give you an injection suppressing your telepathy and giving you the thorazine shuffle.
Drugs that make one more happy while simultaneously making one less able to operate heavy machinery have been around since cave man days. Archeologists suspect that agriculture was invented not to make food but more to make beer. Recreational drugs has been around for many thousands of years, it is not going to go away any time soon.
The legality of such substances is often more a matter of political factors than practicality. The fact that in many western cultures such recreational drugs as tobacco and alcohol remain legal while safer drugs are not is an object lesson. It makes more logical sense to legislate government regulation of controlled substances on the basis of addiction potential or toxic effect. Be that as it may, such political reasons will probably be common in the far future, because some things never change.
A few 1970s era science fiction stories tried to be edgy and shocking by depicting future societies with legal use of marijuana. As I write this sentence in 2019 such edginess is becoming passé due to real-world efforts at legalization.
Occasionally in science fiction such drugs can be weaponized. An example is LSD or other hallucinogen used to impair enemy soldiers by giving them hallucinations. LSD gas bombing is popular.
In Adous Huxley's BRAVE NEW WORLD, the upper crust is kept tranquillized by a perfectly safe euphoric drug called Soma.
In E.E."Doc" Smith's LENSMAN series the dreaded Thionite is an addictive drug which will make the user experience the hallucination of every desire they ever had becoming true. Meanwhile the user's body is in a tetanus-like spasm. The first thing a user wants after coming out of the spasm is another dose, which unfortunately will give you a deadly heart attack. Smart users ensure there are no additional doses within crawling distance.
In the satirical comedy novel Red Dwarf: Infinity Welcomes Careful Drivers by Grant Naylor, there is the recreational drug Bliss. This drug is so addictive that you get hooked by merely looking at it… which makes it very difficult for police to carry our drug busts.
BLOODHYPE
artwork by Bob Eggleton
“Fine! Good!” Orvenalix reached into a drawer and removed a small vial of glass … no, quartz … with a pressure lock twice as big as the container, and a small bit of black board. Kitten and Porsupah slid their chairs closer. Orvenalix keyed the lock and sprinkled, very carefully, a few grains of white crystal onto the board. “Since you’ve both, presumably, `read the manual,’ perhaps you can tell me what this is?” Both junior officers leaned forward.
The Tolian sniffed once, gently. “Odorless. Clear, rhombehedric crystals with a glassy luster.” The Tolian crushed one of the largest pieces to powder in a sharp, trimmed claw. He sniffed again, careful not to inhale the dust. “Concoidal fracture, no odor released on pulverizing … yes, I think I know what it is, Major.” He turned and looked at Kitten. “The lines of fracture turn blue, they turn blue.” Her eyes widened, and she couldn’t help but whisper when she spoke to Orvenalix. “Bloodhype. Very high grade, too, if the fracture line turns that dark.” The antennae dipped slightly. “Almost pure. Also known as faster, brain-up, phinto, silly-salt, and many other names the mere mention of which are sufficient to inspire thoughts of regurgitation among intelligent, feeling beings.” “I thought I read that the Hyperion forests on Annubis were sterilized and wiped out ten years ago,” Kitten said. “As indeed they were,” the intelligence officer continued. “Naturally, that was the first place the Service checked. We found nothing to indicate that any of the plants had survived the holocaust. At that time it was believed that the Hyperion plant could grow only on Arbutus. Transplanting was attempted for scientific purposes, but the seedlings and mature plants died rapidly as soon as they were removed from the planet. Fertilized seeds likewise transshipped did not sprout. In wiping out the supply it turned out that the species had been effectively exterminated for all purposes!” “I wouldn’t imagine anyone raising a fuss over that,” said Porsupah. “Other than a few masochistic botanists, no one did.”
“It seems, though, that someone, somewhere, has gotten hold of some seeds and found a way to make them sprout, and worse, reproduce.” “What sort of … of creature, would want to restart the traffic in bloodhype?” said Kitten, shuddering. “Soft-angles, I remember you to be a brilliant student. Someday I hope you will make an even better agent, but in many ways you are still an immature grub. The galaxy contains a high volume of pure loathsomeness. Of which I have seen far more than is good for one’s sleep. There are plenty of beings nominally labeled ‘intelligent’ who would sell their own eggs, and worse, for a few credits. The thing here that makes me marvel is not the perpetrators, but their science.
“I don’t have to tell you what bloodhype addiction does. These new users display the same symptoms and reactions as those of over a decade ago. Which means that this new strain is at least as powerful as the original. It affects any living creature with a complex neural system and circulating liquid in its body. ‘This includes every known intelligence, with the exception of a few silicon based primitives on restricted planets. Direct injection is the most common method of application, but inhaling the drug in sufficient quantities is also effective. “Concentrating on the neurons, the drug produces an extremely pleasurable sensation. The thing about bloodhype is that most drugs work only on the mind, by distorting and affecting the images it creates and the information it receives. Bloodhype, on the other hand, is more in the nature of direct neural stimulation. In other words, instead of producing distortions in the information-interpreter—the brain—the original information is distorted right at the beginning, at the original nerve pickups in hands, feet, liver — everywhere the blood can carry it. The effect has been described many ways. One addict said it was like being the highest-pitched wire on a stringed instrument. It’s many, many times more powerful than anything that works just on the mind acting as it does directly on the nerve cells rather than the brain. A moderate dose produces a ‘fire-fit’, an intense burning sensation that seems to add to the overall pleasure.
“Withdrawal symptoms commence anywhere from 60hh or 72 t-standard hours after the last injection. Coordination begins to go, accompanied by a speed-up in involuntary muscular reactions. Breathing can speed up or slow, as can the heart and other self-regulating muscles. The senses are badly confused and feed false reports to the brain, which is itself undergoing severe emotional changes, from depression to exaltation and so forth. The body goes downhill like an unhatched egg with insufficient yolk. It’s possible to be in excellent physical shape and be dying—until the final moment, when every thing seems to jump on you at once. “You go slowly insane, aware of what’s taking place all the time. ‘Dying by inches,’ I believe a terran author called something far less extreme. The only way an addict can survive, once hooked, is if the medics can get to him fast. A lot of very complicated and expensive equipment supports the being’s nervous system until the drug has burned itself out. Very painful and not always successful. If the brain itself has been too badly damaged, nothing can be done. In such cases, mercy killings are not unknown. “If 120hh or 144 t-standard hours have passed, there is a ninety-eight and something percent chance of an excruciatingly painful death occurring. In such cases even the best of medical treatment is useless. There is, of course, nothing like a simple antidote.”
(ed note: Virgil Samms is the first Lensman, superman secret agents of the Galactic Patrol. He is operating undercover as Olmstead, trying to discover the source of the deadly drug Thionite. He is trying to infiltrate the criminal organization of Senator Morgan, being interviewed by the flunky Herkimer. )
“I see. You will do, Olmstead, if you live. There’s a test, you know.” “They told me there would be.” “Well, aren’t you curious to know what it is?” “Not particularly. You passed it, didn’t you?” “What do you mean by that crack?” Herkimer leaped to his feet; his eyes, smoldering before, now ablaze. “Exactly what I said, no more and no less. You may read into it anything you please.” Samms’ voice was as cold as were his eyes. “You picked me out because of what I am. Did you think that moving upstairs would make a bootlicker out of me?”
“Not at all.” Herkimer sat down and took from a drawer two small, transparent, vaguely capsule-like tubes, each containing a few particles of purple dust. “You know what this is?” “I can guess.” “Each of these is a good, heavy jolt; about all that a strong man with a strong heart can stand. Sit down. Here is one dose. Pull the cover, stick the capsule up one nostril, squeeze the ejector, and sniff. If you can leave this other dose sitting here on the desk you will live, and thus pass the test. If you can’t, you die.” Samms sat, and pulled, and squeezed, and sniffed.
His forearms hit the desk with a thud. His hands clenched themselves into fists, the tight-stretched tendons standing boldly out. His face turned white. His eyes jammed themselves shut; his jaw-muscles sprang into bands and lumps as they clamped his teeth hard together. Every voluntary muscle in his body went into a rigor as extreme as that of death itself. His heart pounded; his breathing became stertorous. This was the dreadful “muscle-lock” so uniquely characteristic of thionite; the frenzied immobility of the ultimately passionate satisfaction of every desire. The Galactic Patrol became for him an actuality; a force for good pervading all the worlds of all the galaxies of all the universes of all existing space-time continum. He knew what the Lens was, and why. He understood time and space. He knew the absolute beginning and the ultimate end. He also saw things and did things over which it is best to draw a kindly veil, for every desire—mental or physical, open or sternly suppressed, noble or base—that Virgil Samms had ever had was being completely satisfied. EVERY DESIRE.
As Samms sat there, straining motionlessly upon the verge of death through sheer ecstasy, a door opened and Senator Morgan entered the room. Herkimer started, almost imperceptibly, as he turned—had there been, or not, an instantaneously-suppressed flash of guilt in those now completely clear and frank brown eyes? “Hi, Chief; come in and sit down. Glad to see you—this is not exactly my idea of fun.” “No? When did you stop being a sadist?” The senator sat down beside his minion’s desk, the fingertips of his left hand began soundlessly to drum. “But watch now, he’s coming to.”
Samms’ muscles relaxed. He opened his eyes groggily; then, as a wave of humiliated realization swept over his consciousness, he closed them again and shuddered. He had always thought himself pretty much of a man; how could he possibly have descended to such nauseous depths of depravity, of turpitude, of sheer moral degradation? And yet every cell of his being was shrieking its demand for more; his mind and his substance alike were permeated by an overmastering craving to experience again the ultimate thrills which they had so tremendously, so outrageously enjoyed. There was another good jolt lying right there on the desk in front of him, even though thionite-sniffers always saw to it that no more of the drug could be obtained without considerable physical exertion; which exertion would bring them to their senses. If he took that jolt it would kill him. What of it? What was death? What good was life, except to enjoy such thrills as he had just had and was about to have again? And besides, thionite couldn’t kill him. He was a super-man; he had just proved it! He straightened up and reached for the capsule; and that effort, small as it was, was enough to bring First Lensman Virgil Samms back under control. The craving, however, did not decrease. Rather, it increased.
Months were to pass before he could think of thionite, or even of the color purple, without a spasmodic catching of the breath and a tightening of every muscle. Years were to pass before he could forget, even partially, the theretofore unsuspected dwellers in the dark recesses of his own mind. Nevertheless, from the store of whatever it was that made him what be was, Virgil Samms drew strength. Thumb and forefinger touched the capsule, but instead of picking it up, he pushed it across the desk toward Herkimer.
“Put it away, bub. One whiff of that stuff will last me for life.” He stared unfathomably at the secretary, then turned to Morgan and nodded. “After all, he did not say that he ever passed this or any other test. He just didn’t contradict me when I said it.” With a visible effort Herkimer remained silent, but Morgan did not. “You talk too much, Olmstead. Can you stand up yet?” Gripping the desk with both hands, Samms heaved himself to his feet. The room was spinning and gyrating; every individual thing in it was moving in a different and impossible orbit; his already splintered skull threatened more and more violently to emulate a fragmentation bomb; black and white spots and vari-colored flashes filled his cone of vision. He wrenched one hand free, then the other—and collapsed back into the chair. “Not yet—quite,” he admitted, through stiff lips. Although he was careful not to show it, Morgan was amazed—not that the man had collapsed, but that he had been able so soon to lift himself even an inch. “Tiger” was not the word; this Olmstead must be seven-eighths dinosaur.
Soporific drugs, aka "hypnotics", are used to initiate, sustain, or lengthen sleep. They are closely related to sedativesaka tranquilizers, which just calm you down.
Mundanely they are used to treat insomnia, prescribed as "sleeping pills." More importantly some are used as surgical anesthesia.
Criminally they are used as knockout drops or "slipping them a Mickey". The person rendered unconsious can then be robbed or Shanghaied into being an involuntary ship crew member by an evil crimp. In the 1800s chloral hydrate was the popular knockout drops due to its ease of manufacture. In the 1900s the chloroform-soaked rags became common (at least in crime novels).
Stimulant Drugs
Stimulantsaka psychostimulants or "uppers". They induce temporary improvements in either mental or physical functions or both. Effects may include enhanced alertness, wakefulness, and locomotion. They range from caffeine (coffee), amphetamine, cocaine, to methamphetamine (crystal meth).
In Joe Haldeman's THE FOREVER WAR soldiers going too long without sleep can take stimtab, with the understanding that you will pay a metabolic price when it wears off. At that point you can take a second stimtab, but the price increases. You can stay awake and energetic for hundreds of hours on stimtabs but aberrations of judgement and perception snowballed after the second. Eventually you will take freaky hallucinations at face value, and find yourself fidgeting for hours deciding whether to have breakfast.
In David Drake's HAMMER'S SLAMMERS series, the soldiers take a stimulant called a "popper" for the same reasons, and with similar consequences.
In the Space Opera RPG, the drug Tempo will artificially restore lost stamina for 8 hours then for the next 4 hours they are at risk for unexpectedly falling unconscious. The drug Expeditor restores some lost stamina and give artificial extra energy for one hour, after it wears off they are at risk for falling unconscious for the next hour.
MORPHOGEN
"I wish I had slept." He held up a hand as soon as he had said that. "Not that I'm in bad shape. I'm not complaining. Have you ever taken a morphogen?"
"Never heard of it. Is it some kind of drug?"
"Yes. Relatively new. It's not the sleep you need, you know. One doesn't rest in sleep to any greater extent than one would by stretching out comfortably with the eyes open. Less, maybe. It's the dreams we need. We've got to have dreaming time, otherwise cerebral coordination breaks down and you begin to have hallucinations and, eventually, death."
"The morphogen makes you dream? Is that it?"
"Exactly. It knocks you out for half an hour of solid dreaming and then you're set for the day. Take my advice, though, and stay away from the stuff unless it's an emergency."
"Why? Does it leave you tired?"
"No. Not particularly tired. It's just that the dreams are bad. The morphogen vacuums the mind; cleans out the mental garbage-pit accumulated during the day; and it's quite an experience. Don't do it. But, I had no choice. That map had to be prepared and I spent all night at it."
Time Accelerators make the user think and move faster than normal. Everybody around the user appears to be moving in slow motion.
In the RPG Traveller, "Slow" drug accelerates the user's perception and motion by a factor of two (e.g., user can fire their sidearm twice in the time it takes their opponent to fire once) but drug causes medical damage to the user.
The eponymous drug from H. G. Well's The New Accelerator
Scalosian water from the classic Trek episode Wink of an Eye. People under the influence move so rapidly that they cannot be seen. The episode author got the idea from The New Accelerator.
The time accelerator in Arthur C. Clarke's All the Time in the World can speed up a person by a factor of about 500,000. Technically it is a physical device worn on the wrist, not a drug.
Time Decelerators do the opposite, they make the user think and move slower than normal. Everybody around the user appears to be moving like blurs. Note that this will increase the perception of apparent gravity by the same factor. Often the user's body ages at a slower rate as well.
The eponymous drug from Grant Allen's Pausodyne is used for suspended animation, as are many drugs in science fiction used for hibernation/suspended animation for prolonged space flights.
the "Fast" drug from the RGP Traveller slows the user down by a factor of 60:1, it is used for hibernation for space flights. The user is unconsious for the duration and ages at 1/60th of the normal rate.
The S-Space protocol of Charles Sheffield's BETWEEN THE STROKES OF NIGHT slows the user down by a factor of 2,000:1. This means that a trip between stars in a ship moving at 0.1 c only takes a couple of weeks from the standpoint of a person in S-Space mode, but several hundred years from the standpoint of a person in normal mode. Users are conscious, but can only move in free fall or up to a 1/2,000 gravity field.
TEMPUS
artwork by Gene Szafran
I always carry a tube of “tempus fugit” pills; most agents do, as one never knows when giving your reflexes a jolt will get you through a tight spot. Despite the scare propaganda, tempus pills are not habit-forming, not the way the original hashish is. Nevertheless a purist would say I was addicted to them, for I had the habit of taking them occasionally to make a twenty-four hour leave seem like a week. I admit that I enjoyed the mild euphoria which the pills induced as a side effect. Primarily, though, they just stretch out your subjective time by a factor of ten or more, chop time into finer bits so that you live longer for the same amount of clock and calendar. What’s wrong with that? Sure, I know the horrible example story of the man who died of old age in a calendar month through taking the pills steadily, but I took them only once in a while. Maybe he had the right idea. He lived a long and happy life—you can be sure it was happy—and died happy at the end. What matter that the sun rose only thirty times? Who is keeping score and what are the rules anyhow? I prepared it as injections so that it would take hold faster. Ordinarily I watch a clock after I’ve taken tempus; when the second hand stops I know that I’m loaded. But my shack has no clocks and neither of us was wearing ringwatches. It was just sunrise and we had been awake all night, cuddled upon a big low half-moon couch in front of the fireplace. We continued to lie there for a long time, feeling good and dreamy, and I was half considering the idea that the drug had not worked. Then I realized that the sun had stopped rising. I watched a bird fluttering past the view window. If I stared at him long enough, I could see his wings move.
While my hands were being treated and dressed I was brought up to date concerning the period (it turned out to be two weeks) that Mary and I had spent at the cabin. By the Old Man’s orders the doctor gave me a short shot of tempus before he worked on me and I spent the time — subjective, about three days; objective, less than an hour — studying stereo tapes through an over-speed scanner. This gadget has never been released to the public, though I have heard that it is bootlegged at some of the colleges around examination week. You adjust the speed to match your subjective time rate, or a little faster, and use an audio frequency step-down to let you hear what is being said. It is hard on the eyes and usually results in a splitting headache — but it is a big help in my profession.
On a spacecraft where the payload fraction is really tight, they might not have the luxury of bringing along every single medical drug they might conceivably need.
It would be a vast savings in payload mass if the ship can instead bring along some general purpose chemicals and make just the drug that is needed, on demand.
The near-future technology is to use genetically engineered yeast or bacteria in a bioreactor to convert the bacteria food into pharmaceutical product. This is much like the production of beer or wine, but with a more complicated end-product. Penicillin used to be manufactured this way, until they figured out how to synthesize it from scratch. The challenge is designing a bioreactor that will work in free fall.
The far-future technology is to use some form of incredibly advanced 3D printer technology to assemble the medication atom-by-atom via nanotechnology.
Naturally the sickbay crew will have to keep the drug machine under lock and key to prevent some selfish crew member from wasting the precursor chemicals on printing up a batch of recreational chemicals.
BIOMANUFACTURING MEDICINES
An instrument currently aboard the International Space Station could grow E.coli bacteria in space, opening a new path to bio-manufacturing drugs during long term space flights. Research published today in Nature Microgravity used an Earth-bound simulator of the space station instrument to grow E.coli, demonstrating that it can be nurtured with methods that promise to be more suitable for space travel than existing alternatives.
"If we can get microorganisms to grow well in space, astronauts can use them to make pharmaceuticals on demand. This could be vital for survival on long missions where resupplying is not an option." said Richard Bonocora, senior author and a faculty member in the Department of Biological Sciences at Rensselaer Polytechnic Institute. "Here we were asking: 'Is there a better way to grow microorganisms that what is currently being used is space?' And what we find is that —with shear force— yes, there likely is."
With promising results, the team hopes to conduct a similar experiment aboard the space station. And while they're starting with E.coli, the workhorse of molecular biology, the team hopes to eventually use the instrument to grow microorganisms with radiation resistance, which could protect developing pharmaceuticals from the ever-present radiation of space as they are produced.
Bacteria like E.coli need oxygen to grow, and the gold standard method for aerating bacteria in a liquid growth medium uses an orbital shaker, a machine that horizontally shakes a platform on which the vessels containing the liquid can be stowed. The shaker relies on the force of gravity to swirl the liquid contents, which rise and fall within a flask, mixing oxygen with the liquid.
But Bonocora and his research team believe an instrument sent to the space station in July, 2019 could do a better job. Inspired by the research of Rensselaer professor Amir Hirsa, the NASA-built instrument uses shearing force, the force created at the boundary of two bodies pushing in opposite directions from one another, similar to that which occurs at the fault lines between tectonic plates. The instrument uses a syringe to dispense a drop of liquid which forms a bubble. One side of the bubble adheres to a stationary ring, while the other side adheres to a thin ring that can rotate. The rotating ring creates shear force on the surface of the bubble, swirling its contents.
Video Clip "Rensselaer-led Experiment Headed to the International Space Station" click to play video
On Earth, Bonocora used a knife-edge viscometer, an instrument designed by Hirsa's group, in which the tip of a metal tube rotates —similar to the rotating ring in the space-based instrument— at the surface of liquid in a dish to simulate the shearing force. The experiment tested how well bacteria grew when aerated by the knife-edge viscometer and an orbital shaker, with both instruments used at various speeds.
At higher speeds, bacteria aerated by the knife-edge viscometer showed growth rates approaching that of the orbital shaker. Even at lower speeds shear force produced significantly more growth than samples of bacteria that were not mechanically aerated.
"This is a viable way of growing microorganisms. We're starting on a new path, and now we need to think about a more real-life environment, such as on the space station," said Bonocora.
"Space-based pharmaceutical manufacturing is a critical component of our efforts to safely send humans deeper into the solar system. This research is fundamental to that goal," said Curt Breneman, dean of the School of Science. "The successful collaboration between Rick and Amir's teams speaks to our long-standing ties to space exploration, and is one of many examples of the culture of 'low walls' to interdisciplinary research that we are proud to nurture at Rensselaer."
From TECHNIQUE OFFERS PATH FOR BIOMANUFACTURING MEDICINES DURING SPACE FLIGHTS by Mary L. Martialay (2020)
Medical Gear
Real world MARINE 1000 from Adventure Medical Kits. Designed to stabilize patient for up to 12 hours. This is a first-aid kit, not a doctor's bag.
In wilderness areas the crew will carry first-aid kits (containing much more than just a few band-aids and aspirin), and doctors/paramedics will carry portable medical kits. First-aid kits will also be located in damage control storage lockers in strategic parts of the spacecraft or lander.
In Harry Harrison's DEATHWORLD series, people carried little medikits. These require no medical training to use. When pressed over a puncture wound, the infection and poison analyzer will detect toxins and the medikit's tiny computer will automatically select and inject the required antidote(s). Assuming that the user has been vigilant about keeping all the antidote reservoirs filled, of course. Otherwise it will just beep a warning that it is out of the medicine you need, you moron. The user can also press a button to inject a temporary stimulant, though this is for emergency use only. The same goes for the sedation button and pain killer button.
In Larry Niven and Jerry Pournelle's THE GRIPPING HAND, elderly Horace Bury's wheelchair has a "diagnostic sleeve." It also does not require any medical training to use. When put on the arm, the sleeve does a quick automated medical examination including blood tests. The medical computer does a diagnosis and injects medications as required. If it detects a more serious problem it will sound the alert to call a doctor.
In the TV show Earth 2, doctors used a DiaGlove (diagnostic glove). This is a multiple medical tool for use by doctors on their patients, it requires extensive medical and surgical training in order to use. It can check a patient's heart rate, pulse, EKG, temperature, and do several types of blood tests. It can do ultrasound and MRI scans. It has integral tools that a doctor can use for basic surgical functions like laser incisions, cauterizing wounds, and suturing wounds shut. It can even administer defibrillator jolts if the patient suffers a cardiac arrest. It does not do any computerized diagnosis, that is the human doctor's job.
In the RPG Space Opera crew can wear a Personal Medisensor. This is a strap-on wrist unit the same size as a large wristwatch (ask your parents what a wristwatch was, kids). It constantly monitors the physical condition of the user and displays medical data with a holographic display (but it takes medical training to interpret the data). More to the point, if the user suddenly dies, the medisensor automatically injects a dose of Thanokalamine drug to keep their body fresh until their buddies can get them to a hospital with life revival capabilities.
In the RPG ChampionsGadgets! supplement, there was a gadget called an AutoPepper heroes and villains wear on their bodies. If the wearer is knocked unconscious, the autopepper injects stimulants to wake them up and healing drugs to help with damage.
In Frank Herbert's DUNE novels, members of wealthy families prolong their life-span by always scanning their meals with a poison snooper before eating a single bite. The snooper will beep a warning if an enemy (or ambitious offspring) has slipped a deadly poison into the food or drink. This is so common that they have special words for poison placed in food (Chaumas) as opposed to poison placed in drink (Chaumurky). There were hand-held portable poison snoopers for eating on the go, and large models attached to the ceilings of the family dining halls.
The AIR MediKit is a portable diagnostic and treatment device for personal first aid use. Using probes and skin monitors, the MediKit diagnoses the metabolic states of the patient and immediately injects the proper drugs to aid in recovery; analgesics, antitoxins, stimulants, sedatives, etc. This requires no decision at all on the part of the operator who only has to place the Kit against the patient's skin (usually the forearm or thigh area) and press the activate button. Microprocessor intelligence assures proper diagnosis.
Limited to first aid only, the MediKit is nevertheless very effective and reliable as long as it is properly supplied with drugs and chemicals (resupply is available on any world of Tech Level 9 or greater). The Kit constant-ly checks its supply of chemicals and power, and warns the user with "Low" and "Depleted" indicator lights. Another feature of the Kit is the "Trauma" light which indicates that due to MediKit diagnosis, the patient is suffering from serious illness and must be treated by a physician or autodoc immediately. The AIR MediKit is issued with clips to be placed on the owner's belt, and can be recharged in 8 hours at any standard 110 volt power outlet.
In the real world, in 2011 the X Prize Foundation announced the Tricorder X Prize. The constest is to develop a mobile device that can diagnose patients as well as or better than a panel of board certified physicians.
As of 2016, of the 40 teams that initially entered the competition who were reduced to 10 finalists, there are two teams still in the running.
Final Frontier Medical Devices
Dynamical Biomarkers Group
Both contestants are using a mobile device for the brains (since smart phones and tablets are fundamentally small computers) that connect with diagnostic peripherals via Bluetooth (since wires just get tangled up). Both entries have tutorial videos in their mobile device, as well as printed instruction sheets. In theory the devices require zero medical training, just familiarity with smartphones and tablets.
Final Frontier Medical Devices is led by brothers Basil and George Harris, founders of Basil Leaf Technologies. Their tricorder is an iPad Mini talking via Bluetooth with a series of 3D printed diagnostic sensors. component.
Dynamical Biomarkers Group is led by Chung-Kang Peng of the Harvard Medical School. Their tricorder is centered around a box. The box has a modified HTC smartphone on top, and houses several medical sensors that connect to the phone via Bluetooth. Medical sensors include blood-glucose and urine test modules. The box is also the charger for all the sensors, with the box being energized by a standard USB cable. This is because one of the contest rules is the tricorder must be capable of monitoring a patient's vital signs for a full day.
Both entries will be tested over the next few months at the University of California, San Diego and scored. The winner will be announced around mid 2017. Naturally win or lose, both teams plan to bring their product to market, though obtaining certification from the FDA is going to be a nightmare. The XPrize foundation will try to help but against bureaucracy the gods themselves contend in vain.
Dynamical Biomarkers Group might have better luck obtaining certification in China. They have a somewhat less stringent process, and the government would be eager to bring such medical help to the remote regions of the country.
The ScanaduScout, one of the entries in the Tricorder X Prize
The unit is pressed on the patient's temple for ten seconds
Alas, they dropped out of the contest
(ed note: MarkusB is an electronic hobbyist trying to create a simplistic tricorder)
As I have always been fascinated by medical electronics and medical mathematics and was sickened by a thrombosis on left calf a month ago, which nearly killed me because I didn't took the pain and the tumefaction serious for several days, I recently started to develop a simple form of a medical tricoder.
My tricorder has currently only two sensors: an infrared thermometer (MLX90614) to measure the body temperture on the forehead and a PPG (Photoplethysmograph) sensor to measure pulse/heart rate on the ear lobe.
During my research I was astonished, how many medical information can be computed by only knowing the body temperature, pulse rate, gender and age. By far the most interesting discovery was the use of naive Bayes classifier in automated medical diagnosis. Also very interesting are the following fever diagnoses, which are not too difficult to translate into an according algorithm: fever in adults and fever in infants and children.
In Star Trek, doctors use medical tricorders (a tricorder optimized for medical use) to diagnose ailments (the pocket-sized medical scanner is a more portable but does not report as much detail). A device called an anabolicprotoplaser is used to heal wounds by repairing torn veins and arteries and uniting the nerves and muscle fibers using some technobabble radiation. Hyposprays inject medications using jets of air instead of needles, this was cutting-edge science fiction in the time of the original Star Trek but is now common in the real world. In the field Starfleet doctors would carry a medkit containing essential medical tools.
According to the Star Fleet Medical Reference Manual, a medical tricorder has a compartment in the lower section containing a bare-bones emergency surgical kit.
MEDICAL TOOLS
When it comes to surgery, the tool schema is much like that of engineering tools. Surgical tools mainly fall into one of two categories. They cut one thing into two or they join two things into one. They subtract or add (the ancient alchemists called it "Solve et coagula", or analysis and synthesis). In Star Trek, the lasers scalpels cut things into two, and the anabolic protoplasers (somehow) cause body tissues to grow back together. The implication is that the protoplasers somehow use lasers to hyperstimulate anabolism (cell division). Which is total technobabble. In the real world the closest thing to a protoplaser is the skin-cell gun used for burns, but that requires stem cells harvested from the patient.
There are a few tools in other categories: Diagnostic, Measuring, and Supportive. The tricorder and medical scanner is the diagnostic tool (medical database and expert system) and the measuring tool (x-ray and MRI scans). Surgical supportive tools are not shown in Star Trek but in the real world they include retractors, clamps, and forceps. And of course an array of pharmaceutical drugs used to diagnose, cure, treat, or prevent disease.
Surgery is difficult in the field because for best results it requires a sterile area to operate in, and anesthesia for the patient. Star Trek surgical kits include a magic drug called "sterilite" which technobabblically protects the surgical patient from becoming infected when operated on in an unsterile environment. And another magic drug called "melanex" which technobabblically induces safe anesthesia. In the real world, anesthesia is a tricky dangerous procedure that must be closely monitored to prevent harming or killing the patient. The drugs used must be carefully matched to the patient's allergies and genetic make-up.
DEBRIDING GLOVE
(ed note: Debridement is the medical removal of dead, damaged, or infected tissue to improve the healing potential of the remaining healthy tissue. I was going to include a link to the Wikipedia article but the images there were too disturbing.
Mercenaries Churchie and Dwyer were cooking moonshine over a wood fire in the fox hole when their position came under bombardment. To avoid being killed by the bombs they had to lie in the wood fire. Afterwards the medic uses a debriding glove to remove the severely burned tissue to prepare for a coating of spray skin. The medic is curious about how the troopers got the burns, but the troopers are not talking.)
"Well, you might at least give me something for the pain," Churchie grumbled. He lowered himself again onto the cot that doubled as an operating table.
"I'm going to give you something," Bertinelli said. "I'm going to give you a square meter less skin if you don't shut up and lie still." He touched the deep burn over Dwyer's right shoulder blade. The mesh of sensors and tiny hooks in the debriding glove's pad began to purr. Under the control of a microprocessor in the wristlet, the glove was lifting off dead tissue to prepare the area for antiseptic and a covering of spray skin. In the same mild voice, the Corpsman added, "I can see the bombs starting fires and blowing the trash into your shelter. But I'm damned if I see why you thought you had to lie in it. And I'd like to know what you found to bathe in that had such a pong, too."
From THE FORLORN HOPE by David Drake (1984)
TECHNOBABBLE SURGICAL TOOLS
In the techno-magic area, there are many instances of science fictional technology of some kind of technobabble ray that instantly heals wounds that would ordinarily require surgery and a long convalescence. They are all pretty much fantasy, aside from the before-mentioned skin-cell gun.
Other devices emit technobabble rays that instantly cure disease, mostly by using some handwaving way to kill only the harmful bacterial/viruses but leaving untouched the vital microorganisms the body needs to function (such as the digestive bacteria in the colon). Killing all the bacteria could result in massive diarrhea at best, or an exotic death at worse. Perhaps even instant death, since the vital mitochondrion who produce the ATP cell fuel are more or less bacteria that symbiotically live inside the body's cells.
Such an antiseptic ray would have to be aim-able. Intestinal bacteria inside the bowels are vital and should be spared from the antiseptic ray. But the same bacteria released into the abdominal cavity by gastrointestinal perforation (say by a sword or gunshot) can cause death by sepsis. So it would be counterproductive to make the antiseptic ray such that E. coli bacteria are immune.
Star Trek
The previously mentioned Anabolic Protoplaser emits a ray that a surgeon can use to cause tissue, blood vessels and nerves to grow together and merge in seconds. The Dermal Regenerator is a weaker version used to heal minor skin wounds, such as cuts and burns. The Bone-knitting Laser instantly fixes broken bones.
Battlestar Galactica
In the episode Saga of a Star World Dr. Payne uses a colored ray with sparklies from some unnamed machine to heal Cassiopea's broken arm.
Imperial starship sickbays have a piece of equipment called a "regeneration stimulators" that can cause tissue to grow back together. But first you have to surgically remove all the gangrene.
If a raiding Star Wolf space viking gets a minor wound in battle, they just slap a "heal-patch" on it. But for serious injuries, they have to lie under the medical rays of a "heal-lamp".
The "Ready-Knit" helps broken bones to rapidly grow back together
ANABOLIC PROTOPLASER
McCoy's fingers probed lightly around the broken spear shaft that protruded from the boy's side.
"Sara, put a represser on that," he ordered.
The woman removed a small, oblong object and placed it near the wound. She pressed a button on the instrument and, instantly, the flow of blood stopped under the influence of a low-power force-field.
"Suction," McCoy said.
Sara pressed a flexible hose to the wound and the blood was drawn away.
"Now, I can see what I'm doing," McCoy murmured. "Sara, prepare an automatic IV, universal hemo factors, one liter," he ordered a moment later.
Snapping open a small kit, Ensign George removed a telescoping metal rod with a collapsible tripod base. Next, a plastic pouch containing a dark powder was hung at the top of the rod. She poured a liter of water from a storage jug into it. The powder dissolved almost instantly, and a red fluid began to run through a plastic tube into a needle which had been inserted in the boy's left arm.
"Good," McCoy said, his eyes glancing up briefly. "Now a type oh-oh scalpel."
Ensign George handed the instrument to McCoy and he pressed the tip of the slim cylinder against the boy's side. A short, bloodless incision appeared under the ragged hole around the spear shaft.
"Probe," he ordered.
Sara handed him a flexible, light-carrying tube with tiny waldoes on it, and he inserted it into the small incision below the wound. Plugging a lead from the other end into the medical tricorder, he studied the display on the instrument's tiny screen.
"Take a look, Jim."
"Ugly," Kirk said, looking at the black silhouette of the barbed spear point which had torn through the chest muscles and was buried in spongy gray lung tissue. "How are you going to get that thing out?"
"Watch. Minilaze, Sara," he ordered.
She handed him the tiny cutting tool. He made a clean incision through the tissue that had closed in around the barbs, the beam cauterizing as it cut. Then, grasping hold of the short, splintered stub, he gently pulled the head out.
"Sara, anabolic protoplaser, type zero." He applied the tip of the instrument to the interior of the wound, slowly working it outward to repair torn veins and gashed arteries, and unite nerves and muscle fibers. Soon, all that was left was the closing of the jagged tear where the spear had gone in and the small incision below it.
"Type two protoplaser."
"Bones, wait," Kirk said, breaking his long silence. "I have the impression this is the boy's first battle; he only looks about fourteen or fifteen."
"So?" McCoy asked.
"How about giving him something to remember?"
"Like old Heidelberg, eh?"
"Something like that, Bones."
"If Starfleet finds out, they may lift my license," McCoy said, adjusting the protoplaser and setting to work.
When he finished, he looked at a puckered scar that made a semicircle on the boy's chest where the shaft had been. He made a quick scan with the medical tricorder and then switched it off.
"That'll give him some status with the other boys," he said. "And with a little rest, some hot soup, he'll be back on his feet in a day or two. Now the head wound."
He studied the torn flesh critically. "Good thing they shave their heads. Saves me the trouble of depilating him."
When he had finished, McCoy injected Alt with another dose of universal antibiotic and a stimulant to counteract the anesthesia. By the time the boy began to come around, the Federation medikit was safely back in its hidden compartment.
From SPOCK, MESSIAH! by Theodore Cogswell and Charles Spano (1976)
DIRECT IN-MUSCLE BIOPRINTING
In vivo handheld bioprinting of the novel Muscle Ink (Courtesy: Adv. Healthcare Mater. 10.1002/adhm.202002152)
(ed note: Paging Dr. McCoy, your Anabolic Protoplaser has arrived—)
What prize do you get for not moving a single muscle all week? A trophy!
Alternatively, patients who have undergone volumetric muscle loss injuries may be interested in a novel technology recently reported in Advanced Healthcare Materials. The authors of the article – from the University of Nebraska, the University of Connecticut and Brigham and Women’s Hospital – developed a handheld printer to deliver hydrogel-based bioinks for treatment of such injuries.
When a large proportion of a muscle’s mass is lost, due to trauma, disease or surgery, the muscle begins to repair itself in such a manner that disabling scar tissue left behind causes loss of some degree of muscle function. Numerous approaches to assist the body’s natural regenerative processes have been developed, but all have limited efficacy and utility. For example, treatments such as direct cell delivery are constrained by the complex process of differentiating and harvesting myogenic cells, the cells that evolve into skeletal muscle. In settings where a direct and rapid response to volumetric muscle injuries is required – specifically in military trauma care – such approaches are inapplicable.
This latest study demonstrates a feasible approach for treating such injuries. The researchers developed a novel “Muscle Ink” for printing directly into large muscle-loss wounds. Within this specialized ink, vascular endothelial growth factor – key to inducing the angiogenesis and vascularization needed for muscular regeneration – is attached to 2D nanoclay discs, allowing for its continuous release over multiple weeks. The team incorporated these growth factor-bound discs into a biocompatible hydrogel that can adhere to wet tissue, such as the remaining musculature. The resulting scaffold has mechanical properties conducive to cellular regeneration and natural deformation during movement.
The gel is applied by loading it into a novel handheld printer, composed of a loadable syringe, a motor-controlled syringe pump and an ultraviolet light-emitting diode for in vivo hydrogel crosslinking. Clinicians can utilize the device for hot glue gun-like printing directly into wounds, creating a scaffold for cell regeneration and an environment that induces the same.
Left: the handheld printer. Right: murine model bioprinting. (Courtesy: Adv. Healthcare Mater. 10.1002/adhm.202002152)
The researchers evaluated the efficacy of the printing process in murine models. Animals underwent muscle mass injuries to the quadriceps. Some were left untreated, while others were treated with the Muscle Ink, with or without growth factor. After an eight-week recovery, the animals were tested for running function.
The mice treated with growth factor-loaded Muscle Ink had a maximum running speed insignificantly different from that of uninjured mice. This group was also able to run approximately twice as far as the untreated group or those with Muscle Ink but without growth factor. This test supports the premise that slow release of growth factor by the ink was responsible for the improvement in functional performance after volumetric loss muscle injury.
The research team envisions that, in addition to the tested skeletal muscle, this printing technique could be applied for treatment of other soft-tissue wounds. The handheld printer helps broaden the potential of in vivo delivery of hydrogel scaffolds for tissue therapy.
A handheld “biopen” capable of 3D printing cartilage tissue could for the first time be used during surgery to treat cartilage injuries and osteoarthritus. The extrusion-based device, which prints live stem cells embedded in a hydrogel material, produces constructs that look and behave just like natural articular tissue (Biofabrication10045006).
“This is in stark contrast to conventional reparative cartilage made of fibrocartilage, which is very different in structure to physiological cartilage, inferior in quality and not durable,” say the researchers, a multidisciplinary team that includes surgeons, biologists, physicists and engineers. “Our technique and the scaffolds we are able to produce provide much hope for treating patients suffering from cartilage injuries and osteoarthritis.”
Cartilage is a highly specialized tissue that has so far proved difficult to replicate using conventional tissue engineering techniques. Its special mechanical properties arise from the fact that it contains only a few cells, does not contain blood vessels, and has a distinct 3D collagen fibre structure comprising aggregated proteoglycans in an organized matrix.
While some success has been reported for surgical treatments that exploit engineered cartilage tissue, existing procedures require two separate operations: one to remove the damaged tissue, and another to replace the tissue once it is repaired. What’s more, surgeons report a high failure rate – partly because pre-fabricated scaffolds might not perfectly match the defect, and partly because the implanted tissue is not similar enough to natural cartilage to survive for long inside the body.
Researchers believe that treatments using human stem cells could offer a solution, but few studies have been reported to date. In this new work, reported in the journal Biofabrication, scientists from the University of Melbourne, the University of Wollongong and the St Vincent’s Hospital of Melbourne provide in vitro evidence that their new biopen could enable human stem cells to be 3D printed inside the operating theatre. The ultimate aim is to enable surgeons to “sculpt” patient-specific structures in real time, creating scaffolds that perfectly match the geometry of the defect and achieve the best possible contact between the bioscaffold and the host tissue.
The team tested their approach with human-derived mesenchymal stem cells (hADSCs) that had been harvested from the infra-patellar fat pad of donor patients with osteoarthritis. Once the stem cells had been embedded in a hydrogel material, the resulting bioink could be extruded through the biopen to create a cell-laden bioscaffold.
One key feature of the new biopen is a specially designed nozzle that allows cells and biomaterials contained in separate cartridges to be extruded co-axially. The inner core of the extruded material contains live stem cells, while the outer shell contains cross-linked material that provides rigidity to the printed construct.
In this study the researchers used the biopen to print 3D scaffolds laden with stem cells, which were then cultured in vitrofor eight weeks in the presence of cartilage-forming media. “Thanks to a series of sophisticated histological, molecular and imaging techniques, we confirmed that the tissue that developed within the constructs forms, appears, and behaves like articular cartilage,” say the researchers. “This material is expected to be as durable as real cartilage.”
This detailed in vitro analysis is a crucial step towards full-scale clinical trials. The group has already shown that the device could be used in a real-world setting through preliminary in vivo experiments in a large animal model, and more extensive in vivo testing will be needed before the biopen can be tested on humans.
At the same time, the researchers are investigating whether the same technology could be applied to other organs and clinical scenarios, while also looking at ways to speed up and streamline the processes needed during surgery.
“We are refining our methodology to upscale the production of the inks used in the device, and to fine-tune how to harvest and prepare the mesenchymal stem cells,” they say. “We are also aiming to develop a protocol that will enable one-step harvesting, preparation and delivery of the cells during surgery.”
"You have a renewer ray?" he asked, drawing his arm out of the sling. "We have. How long it will continue to function locked to these city currents is another question. We cannot be sure of anything. I am Medico Lasilo Tre. A break?" His fingers were already busy about Kartr's wrist, unfastening the bandages Zinga had put on that morning. "I don't know. Ah—" Kartr sucked in his breath as Tre began probing the bruised and purple flesh. Then the ranger was pushed down on a stool at the edge of the renewer beam, his throbbing arm stretched out under the concentrated ray, feeling again the draw of those invisible healing motes. Twice Tre snapped off the current and came to examine the hurt with delicate finger tips—only to turn it on again after shaking his head. The third time he was satisfied. Kartr lifted his arm gingerly and flexed first his fingers and then his wrist. Although he had once before been under the ray—to renew a leg almost chewed to pieces—the wonder of the restoration was as great as ever. He pulled off his sling and grinned happily at the medico.
They had to send for a surgeon's mate to undress him. The medic snipped at the armor cloth embedded in his left arm and muttered. "Hold still, sir. That arm's cooked good." His voice was disapproving. "You should have been in sick bay a week ago."
"Hardly possible," Rod answered. A week before, MacArthur had been in battle with a rebel warship, who'd scored more hits than she ought to have before surrendering. After the victory Rod was prize master in the enemy vessel, and there weren't facilities for proper treatment there. As the armor came away he smelled something worse than week-old sweat. Touch of gangrene, maybe.
"Yes sir." A few more threads were cut away. The synthetic was as tough as steel. "Now it's gonna take surgery, Commander. Got to cut all that away before the regeneration stimulators can work.
Medical scanner from ST:TOS. Scan data is reported to the doctor by a series of warbling tones, and by an array of scales on the "readings dial". Image from Star Trek Star Fleet Technical Manual (1975)
Spray applicator from ST:TOS. Used for spray-on bandages and topical medication. Standard vial contains blood coagulant/antiseptic/bandage mix Image from Star Trek Star Fleet Technical Manual (1975)
Medical Accessory Kit Apollo 11 Command Module The kit has three component layers fitted with medical supplies and small medical equipment. It contains motion sickness injectors, pain suppression injectors, a two ounce bottle first aid ointment, one-ounce bottles of eye drops, nasal sprays, compress bandages, adhesive bandages, an oral thermometer and spare crew biomedical harnesses. Pills in the medical kit include antibiotics, nausea, stimulant, pain killer, decongestant, diarrhea, aspirin and sleeping.
Apollo Medical Accessories Kit
Constant Wear Garment Harness Plug
3
ECG Sponge Packages
14
Electrode Bag
1
Electrode Attachment Assembly
100
Micropore Disc
50
Sternal Harness
3
Axillary Harness
1
Electrode Paste
1
Oral Thermometer
1
pH Paper
1
Urine Collection Roll-On Cuffs
6
Lunar Module Medical Kit
Rucksack
1
Stimulent Pills (Dexedrine)
4
Pain Pills (Darvon)
4
Decongestan Pills (Actifed)
8
Diarrhea Pills (Lomotil)
12
Aspirin
12
Band-Aids
6
Compress Bandages
2
Eye Drops (Methylcellulose)
1
Antibiotic Ointment (Neosporin)
1
Sleeping Pills (Seconal)
6
Anesthetic Eye Drops
1
Nose Drops (Afrin)
1
Urine Collection Roll-On Cuffs
6
Pronestyl
12
Injectable Drug Rucksack
1
ID Kit Cardiac (Lidocaine)
8
INSIDE THE AID BAG OF A U.S. ARMY COMBAT MEDIC
KipKaro, medic in the U.S. Army, displays the contents of a combat medic's bag (go to his imgur album to see the full-sized images). Naturally it is optimized for medical emergencies commonly encountered on a battlefield.
This is the aid bag from a deployment to Afghanistan with an infantry battalion in the last five years. The aid bag is worn on the back of the combat medic, along with all the other gear. Modern medics carry the same M4/M16 as everybody else.
How you set up your aid bag is mostly up to the individual. We are encouraged to do whatever works best for us. I attached four pouches to the sides of my aid bag, and have labeled them with their contents. The labels are just in case somebody else needs to use my aid bag, but each medic knows his own bag well enough that it wouldn't matter if he was blindfolded.
The upper pouch is labeled TQ, which is the abbreviation for tourniquet. The military uses Combat Application Tourniquets, which we call CAT's or CAT tourniquets. This tourniquet is the only medical intervention that can be performed under fire. Everything else has to wait until the enemy is taken care of.
The CAT has strong velcro on the straps, which are looped around a limb and pulled tightly. The windlass (bar) is then turned until it cannot be turned any more, and then it gets fit into one of those clips on the left. This cuts off all blood flow to the extremity.
The lower pouch is marked with a circled H, which stands for hemorrhaging. This pouch contains equipment that you would need to control serious arterial hemorrhaging that cannot be controlled by a tourniquet, such as on the neck.
Combat Gauze is gauze that is impregnated with a hemostatic agent, which clots blood on contact. For a gunshot to the neck, the wound is packed with combat gauze, and if the bleeding is controlled, it is packed the rest of the way with regular gauze and firmly held in place with the ace wrap.
The other side of the aid bag
The top pouch contains Emergency Trauma Bandages (ETB's).
Open the ETB's plastic wrapper and you'll find another plastic wrapper. These are sterile on the inside and so we can use them for chest seals if we run out of regular chest seals (more on that later).
The ETB comes rolled up
This side to wound. You roll the ETB tightly around the limb, and the banana shaped buckle there helps pull it tight.
The end of the roll has clips that clip onto itself.
The other pouch has chest seals and nasopharyngeal airways (NPA's).
The chest seals are basically big, super sticky stickers. A penetrating wound to the chest cannot be controlled with a tourniquet, and internal bleeding can't be compressed with an ace wrap. The chest seals cover up the wound to prevent any air from entering the chest, which can collapse the lung.
The NPA (green thing) is a tube that gets lubed up and shoved into the casualty's nose. They keep the airway open if the casualty loses consciousness.
The inside of the aid bag, with everything folded in
Pockets fold out
The pockets are labeled with big letters, "H A B C", which any medic would recognize as "Hemorrhaging, Airway, Breathing, Circulation", the major threats to life and the things we look at first, in that order.
This is the same thing as the pouch on the outside. Hemorrhaging is very important, so more is better.
Here is the Airway stuff. I don't have a King LT anymore, but they were basically a big tube that we shove down somebody's throat to keep their airway open.
You already have seen the NPA. This one has some lubrication to go with it. If no lube is available, you use the casualty's spit.
The other thing is the cricothyroidotomy kit, aka cricothyrotomy kit, aka cric' kit, contains tools for making an incision in a casualty's neck and inserting an airway tube directly into the trachea.
Breathing and Circulation on the other side. I only got one bag valve mask (BVM), and after it got covered in blood I didn't get another one. I'm sure you've seen them in TV shows. They are the bags that people squeeze to breathe for a person.
This is the needle and catheter for a needle chest decompression (NCD). If air gets into the chest outside of the lungs, it makes it harder for the lung to inflate. Too much air collapses the lung. The treatment is to seal off all chest wounds with the chest seal and stick a big needle in the chest to drain the extra air.
Inside the tube is the needle and catheter. That whole thing goes straight down into the chest, about an inch lower than the clavicle. the needle comes out, but the plastic catheter stays in.
This is what is in the Circulation pouch. Those two kits contain everything you need to start an IV, except for the fluids of course. What's missing from here is a sharps container, which is a little tube for storing the used needles after you're done with them.
Back of the IV kit
The rest of the aid bag. There are a few new things.
That black thing is a glove, which is stuffed with other gloves in pairs of two.
This is an abdominal ETB. It works the same way as the smaller ones.
1" medical tape. The end is taped to itself for quick use, and that cord is held together with a single piece of tape, so it breaks quickly if I need the tape in a hurry.
Not pictured is the 3" tape, which is one of the most important pieces of equipment a medic has. Before i used it all, I had it set up in the same way.
This is a FAST 1, a sternal intraosseous device. If we are unable to get an IV in a casualty (for example if they were a quad amputee or were in so much shock that the veins were all collapsed), we use this thing to go straight into the sternum. We will actually deliver the same fluids, but instead of going into a vein, it goes directly into the bone in the middle of your chest.
Epi pen
This is a cravat, which is a green, triangular bandage. It can be used to make a sling, but is often 'acquired' for use as a bandanna.
SAM splints. These are made of a flexible sheet of metal covered in foam. When they are curved, they become really stiff and are perfect for splints.
They can be molded to any person for any wound on any limb
The rest of this stuff is just band aids and over the counter stuff for cuts, scrapes, and bruises.
Med Unit from The Morrow Project RPG
The Med unit is a large enclosed bed with attached medical support equipment. It is normally found in bases and in the MARS-One and Scientific-One vehicles. The unit is self-contained and may be used as an operating theater with a sterile environment. The med unit is attached to a bio-comp for automatic diagnosis and treatment. The unit can also be used as a freeze-tube for cold sleep.
"Autodoc" is short for "automatic doctor". It is a science-fictional high tech device shaped like a coffin that a patient enters. Once inside a medical computer diagnoses the patient and cures with the administration of appropriate medication and/or surgery. Just the thing if you cannot afford a real human doctor. Or for an army support ship that expects to be tasked with handling sudden influxes of large numbers of casualties.
They would be incredibly useful, but they do not exist in the real world, nor are they likely to exist anytime soon. No only are the technological challenges daunting, but liability insurance will make them prohibitively expensive until it is proven they have a higher success rate than human doctors. Whereupon they will face stiff resistance from human doctors facing job loss.
Autodocs appear in The Ethics of Madness by Larry Niven, A Plague of Demons by Keith Laumer, The Polity novels of Neal Asher, and the Liaden Universe novels by Sharon Lee and Steve Miller.
A PLAGUE OF DEMONS
“Emergency override!” it said sharply. “Sensing instruments indicate you require immediate medical attention.” There was a sound behind me; I turned. As if in a dream, I saw a white-sheeted cot deploy from a wall recess, roll across the room, hunting a little, then come straight on and stop beside me. “Place yourself on the cot, with your head at the equipment end.” The voice echoed from far away. I made a vast effort, pushed myself clear of the chair, fell across the bed. I was struggling to get myself on it when I felt a touch, twisted to see padded, jointed arms grasp me and gently but firmly hoist me up and lay me out, facedown. The sheet was smooth and cool under my face. “You will undergo emergency diagnosis and treatment,” the voice said. “An anesthetic will be administered if required. Do not be alarmed.” I caught just one whiff of neopolyform; then I was relaxing, letting it all go, sliding down a long, smooth slope into dark sea.
Two bosomy angels with hands like perfumed flower petals were massaging my weary limbs and crooning love songs in my ears, while not far away someone was cooking all my favorite dishes, making savory smells that put just that perfect edge on my appetite. The cloud I was lying on was floating in sunshine, somewhere far from any conceivable discord, and I lay with my eyes closed and blissfully enjoyed it. I deserved a rest, I realized vaguely, after all I’d gone through — whatever that was. It didn’t seem important. I started to reach out to pat one of the angels, but it was really too much trouble … There was a twinge from my left arm. I almost remembered something unpleasant, but it eluded me. The arm pained again, more sharply; there seemed to be only one angel now, and she was working me over in a businesslike way, ignoring my efforts to squirm free. The music had ended and the cook had quit and gone home. I must have slept right through the meal; my stomach had a hollow, unloved feeling. That angel was getting rougher all the time; maybe she wasn’t an angel after all; possibly she was a real live Swedish masseuse, one of those slender, athletic blonde ones you see in the pictonews — Ouch! Slender, hell. This one must have weighed in at a good two-fifty, and not an ounce of fat on her. What she was doing to my arm might be good for the muscle tone, but it was distinctly uncomfortable. I’d have to tell her so — just as soon as this drowsy feeling that was settling over me went away … It had been a long trip, and the jogging of the oxcart was getting me down. I could feel burlap against my face; probably a bag of potatoes, from the feel of the lumps. I tried to shift to a more comfortable position, but all I could find were bard floorboards and sharp corners. I had caught my arm under one of the latter; there must have been a nail in it; it caught, and scraped, and the more I pulled away the more it hurt —
My eyes came open and I was staring at a low, gray-green ceiling perforated with tiny holes in rows, with glare strips get every few feet. There were sounds all around: busy hummings and clicks and clatters. I twisted my head, saw a panel speckled over with more lights than a used heli-lot, blinking and winking and flashing in red, green, and amber … I lowered my sight. I saw my arm, held out rigidly by padded metal brackets. Things like dentists’ drills hovered over it, and I caught a glimpse of skin pinned back like a tent-fly, red flesh, white bone, and the glitter of clamps, set deep in a wound like the Grand Canyon. “Your instructions are required,” a deep, uninflected voice said from nowhere. “The prognosis computed on the basis of inmediate amputation is 81 percent positive. Without amputation, the prognosis is 7 percent negative. Please indicate the course to be followed.” I tried to speak, got tangled up in my tongue, made another effort. “Wha’s … that… mean … ?” “The organism will not survive unless the defective limb is amputated. Mutilation of a human body requires specific operator permission.” “Cu’ … my arm … off … ?” “Awaiting instructions.” “Die… ‘f you don’t… ?” “Affirmative.” “Permission… granted…” “Instructions acknowledged,” the voice said emotionlessly. I had time to get a faint whiff of something, and then I was gone again …
This time, I came out of it with a sensation that took me a moment or two to analyze — a cold-water, gray-skies, no-nonsense sort of feeling. For the first time in days — how many I didn’t know — the fine feverish threads of delirium were lacking in the ragged fabric of my thoughts. I took a breath, waited for the familiar throb of pain between my temples, the first swell of the sea-sickness in my stomach. Nothing happened. I got my eyes open and glanced over at my left arm; it was strapped to a board, swathed in bandages to the wrist, bristling with metal clips and festooned with tubing. I felt an unaccountable surge of relief. There had been a dream — a fantastic dialogue with a cold voice that had asked… In sudden panic, I moved the fingers of the hand projecting from the bandages. They twitched, flexed awkwardly. With an effort, I reached across with my right hand, touched the smooth skin of the knuckles of the other … Under my fingers, the texture was cool, inhumanly glossy — the cold gloss of polyon. I raked at the bandages, tore them back - An inch above the wrist, the pseudoskin ended; a pair ot gleaming metal rods replaced the familiar curve of my forearm. A sort of animal whimper came from my throat. I clenched my lost fist — and the artificial hand complied.
The boy Rick wrangles a zeowhale artwork by Kelly Freas
(ed note: The good ship Shark is a hydrofoil boat that manages schools of synthetic organisms called "zeolite whales" or zeowhales. These harvest copper and other elements by straining seawater. Marco Mancini is the on-board molecular mechanic. Rick Stubbs is an 18 year old working off his standard 2 year labor draft requirement so as to be eligible for higher education.)
“It’s still handy, though, to know how to work with the
real thing (DNA backbone instead of synthetic zeolite) —after all, you know as well as I do that the
reason you have a life expectancy of about a hundred and
fifty years is that your particular gene pattern is on file in
half a cubic meter of zeolite mesh in Denver under a nice
file number …”
“026-18-5633” muttered the boy under his breath.
“ … which will let any halfway competent molecular
mechanic like me grow replacement parts and tissues if
and when you happen to need them.”
“I know all that, but it still seems dangerous to poke
around making little changes in ordinary life forms,” replied Rick. “There must be fifty thousand people like you in
the world, who could tailor a dangerous virus, or germ,
or crop fungus in a couple of weeks of lab and computer
work, and whose regular activities produce things like that
iron-feeder which can mutate into dangerous by-products.”
“It’s also dangerous to have seven billion people on the
planet, practically every one of whom knows how to light a
fire,” replied Mancini. “Dangerous or not, it was no more
possible to go from Watson and Crick(this injustly ignores the vital contributions of Rosalind Franklin) and the DNA
structure to this zeowhale without the intermediate development than it would have been to get from the Wright
brothers and their powered kite to the two-hour transatlantic ramjet without building Ford tri-motors and DC-3’s
in between. We have the knowledge, it’s an historical fact
that no one can effectively destroy it, so we might as well
use it. The fact that so many competent practitioners of the
art exist is our best safeguard if it does get a little out of
hand at times.”
The boy looked thoughtful.
“Maybe you have something there,” he said slowly. “But
with all that knowledge, why only a hundred and fifty
years? Why can’t you keep people going indefinitely?”
“Do you think we should?” Mancini countered with a
straight face. Rick grinned.
“Stop ducking. If you could, you would—for some people anyway. Why can’t you?” Mancini shrugged.
“Several hundred million people undoubtedly know the
rules of chess.” He nodded toward the board on Dandridge’s control table. “Why aren’t they all good players?
You know, don’t you, why doctors were reluctant to use
hormones as therapeutic agents even when they became
available in quantity?”
“I think so. If you gave someone cortisone it might do
what you wanted, but it might also set other glands going
or slow them down, which would alter the levels of other
hormones, which in turn … Well, it was a sort of chain
reaction which could end anywhere.”
“Precisely. And gene-juggling is the same only more so.
If you were to sit at the edge of the hatch there and let Gil
close it on you, I could rig the factors in your gene pattern
so as to let you grow new legs; but there would be a
distinct risk of affecting other things in your system at the
same time. In effect, I would be taking certain restraints
which caused your legs to stop growing when they were
completed off your cell-dividing control mechanisms—the
sort of thing that used to happen as a natural, random
effect in cancer. I’d probably get away with it—or rather,
you would—since you’re only about nineteen and still
pretty deep in what we call the stability well. As you get
older, though, with more and more factors interfering
with that stability, the job gets harder—it’s a literal juggling act, with more and more balls being tossed to the
juggler every year you live.
“You were born with a deep enough stability reserve to
keep yourself operating for a few decades without any
applied biochemical knowledge; you might live twenty
years or ninety. Using the knowledge we have, we can play
the game longer; but sooner or later We drop the ball. It’s
not that we don’t know the rules; to go back to the chess
analogy, it’s just that there are too many pieces on the
board to keep track of all at once.”
Stubbs shook his head. “I've never thought of it quite
that way. To me, it’s always been just a repair job, and I
couldn’t see why it should be so difficult.”
Mancini grinned. “Maybe your cultural grounding
didn’t include a poem called the ‘Wonderful One-Hoss
Shay.’ Well, we’ll be a couple of hours getting back to the
Guppy. There are a couple of sets of analysis runs sitting
with us here. Maybe, if I start trying to turn those into
language you can follow, you’ll have some idea of why the
game is so hard before we get there. Maybe, too”—his
face sobered somewhat&mdash“you’ll start to see why, even
though we always lose in the end, the game is so much fun.
It isn’t just that our own lives are at stake, you know; men
have been playing that kind of game for two million years
or so. Come on.”
(ed note: The hydrofoil boat proceeds to full speed of sixty-five knots [120 kph or 75 mph]. Abruptly, a rogue steel-eating bacteria finishes chewing through the starboard aft hydrofoil leg, causing a catastrophic failure. The boat smacks into the water and does a cartwheel before coming to rest. The entire crew has severe injuries.)
His words, as it happened, were getting out (Mancini had no idea if the emergency radio was transmitting). The Conger, the nearest of the Shark’s sister fish-tenders, had
already started toward them; she had about forty kilometers to come. On the Guppy the senior mechanic had
fulfilled Mancini’s prediction; he had already made contact
with Denver, and Rick Stubbs’ gene code was about to
start through the multiple-redundant communication channels used for the purpose—channels which, fortunately,
had just been freed of the saturation caused by a serious
explosion in Pittsburgh, which had left over five hundred
people in need of major repair. The full transmission
would take over an hour at the highest safe scanning rate;
but the first ten minutes would give enough information,
when combined with the basic human data already in the
Guppy’s computers, to permit the synthesis of replacement
blood.
(ed note: The crew is rescued and taken to a hospital.)
In spite of tradition, Rick Stubbs knew where he was
when he opened his eyes. The catch was that he hadn’t the
faintest idea how he had gotten there. He could see that he
was surrounded by blood-transfusion equipment, electronic circulatory and nervous system monitoring gear,
and the needle-capillary-and-computer maze of a regeneration unit, though none of the stufi seemed to be in operation. He was willing to grant from all this that he had been
hurt somehow; the fact that he was unable to move his
head or his right arm supported this notion. He couldn’t
begin to guess, however, what sort of injury it might be or
how it had happened.
He remembered talking and working with Mancini at
the latter’s lab bench. He could not recall for certain just
what the last thing said or done might be, though; somehow the picture merged with the foggy struggle back to
consciousness which had culminated in recognition of his
surroundings.
He could see no one near him, but this might be because
his head wouldn’t turn. Could he talk? Only one way to
find out. “Is anyone here? What’s happened to me?” It didn’t
sound very much like his own voice, and the effort of
speech hurt his chest and abdomen; but apparently words
got out. “We’re all here, Rick. I thought you’d be switching back
on about now.” Mancini’s face appeared in Stubbs’ narrow
field of vision. “We’re all here? Did everyone get hurt somehow? What
happened?” “Slight correction—most of us are here, one’s been and
gone. I’ll tell you as much as I can; don’t bother to ask
questions, I know it must hurt you to talk. Gil was here
for a while, but he had just had a few bruises and is back
on the job. The rest of us were banged up more thoroughly. My right leg was a jigsaw puzzle; Bert had an
interesting time with it. I thought he ought to take it off
and start over, but he stuck with it, so I got off with five
hours of manual repair and two in regeneration instead of
a couple of months hooked up to a computer. I’m still
splinted, but that will be for only a few more days. “No one knows yet just what happened. Apparently the
Shark hit something going at full clip, but no one knows
yet what it was. They’re towing her in; I trust there’ll be
enough evidence to tell us the whole story.” “How about the other fellows?” “Ishi is plugged in. He may need a week with computer
regeneration control, or ten times that. We won’t be able
to assess brain damage until we find how close to consciousness he can come. He had a bad skull fracture. The
captain was knocked out, and some broken ribs I missed
on the first-aid check did internal damage. Bert is still
trying to get him off without regeneration, but I don't
think he’ll manage it.” “You didn’t think he could manage it with you, either." “True. Maybe it’s just that I don’t think I could do it
myself, and hate to admit that Jellinge is better at my own
job than I am.” “How about Joe?” “Both arms broken and a lot of bruises. He’ll be all
right. That leaves you, young fellow. You’re not exactly a
critical case, but you are certainly going to call for professional competence. How fond are you of your fingerprints?” “What? I don’t track.” “Most of your right hand was sliced off, apparently by
flying glass from my big culture flask. Ben Tulley from the
Conger, which picked us up, found the missing section and
brought it back; it’s in culture now.” “What has that to do with fingerprints? Why didn’t you
or Mr. Jellinge graft it back?” “Because there’s a good deal of doubt about its condition. It was well overan hour after the accident before it
got into culture. You know the sort of brain damage a few
minutes without oxygen can do. I know the bone, tendon,
and connective tissue in a limb is much less sensitive to that
sort of damage, but an hour is a long time, chemically
speaking. Grafting calls for healing powers which are
nearly as dependent on genetic integrity as is nerve activity; we’re just not sure whether grafting is the right thing
to do in your case. It’s a toss-up whether we should fasten
the hand back on and work to make it take, or discard it
and grow you a new one. That’s why I asked how much
you loved your fingerprints.” “Wouldn’t a new hand have the same prints?” “The same print classification, which is determined genetically, but not the same details, which are random.” “Which would take longer?” “If the hand is in shape to take properly, grafting would
be quicker—say a week. If it isn’t, we might be six or eight
times as long repairing secondary damage. That’s longer
than complete regeneration would take.” “When will you start?” “As soon as I’ve had some sleep. Your blood is back to
normal, your general pattern is in the machine; there’s
nothing else to hold us up. What sort of books do you
like?” “Huh?”
“That head’s going to be in a clamp for quite a while.
You may or may not like reading, but the only direction
you can look comfortably is straight up. Your left hand
can work a remote control, and the tape reader can
project on the ceiling. I can’t think of anything else to
occupy you. Do you want some refreshing light fiction, or
shall I start you on Volume One of ‘Garwood’s Elementary Matrix Algebra for Biochemists?’ ”
A regeneration controller is a bulky machine, even
though most of it has the delicacy and structural intricacy
possible only to pseudolife—and, of course, to “real” life.
It’s sensors are smaller in diameter than human red blood
cells, and there are literally millions of them. Injectors and
samplers are only enough larger to take entire cells into
their tubes, and these also exist in numbers which would
make the device a hopeless one to construct mechanically.
Its computer-controller occupies more than two cubic
meters of molecular-scale “machinery” based on a synthetic zeolite framework. Mating the individual gene record needed for a particular job to the basic computer
itself takes nearly a day; it would take a lifetime if the job
had to be done manually, instead of persuading the two to
“grow” together.
Closing the gap between the optical microscope and the
test tube, which was blanketed under the word “protoplasm” for so many decades, also blurred the boundary
between such initially different fields as medicine and factory design. Marco Mancini and Bert Jellinge regarded
themselves as mechanics; what they would have been called
a few decades earlier is hard to say. Even at the time the
two had been born, no ten Ph.D.’s could have supplied the
information which now formed the grounding of their
professional practice.
When their preliminary work—the “prepping”—on
Rick Stubbs was done, some five million sensing tendrils
formed a beard on the boy’s face, most of them entering
the skin near the edges of the injured portions. Every five
hundred or so of these formed a unit with a pair of larger
tubes. The sensors kept the computer informed of the
genetic patterns actually active from moment to moment in
the healing tissue—or at least, a statistically significant
number of them. Whenever that activity failed to match
within narrow limits what the computer thought should be
happening, one of the larger tubes ingested a single cell
from the area in question and transferred it to a large
incubator—“large” in the sense that it could be seen
without a microscope—just outside Rick’s skin. There the
cell was cultured through five divisions, and some of the
product cells analyzed more completely than they could be
inside a human body. If all were well after all, which was
quite possible because of the limitations of the small sensors, nothing more happened.
If things were really not going according to plan, however, others of the new cells were modified. Active parts
of their genetic material which should have been inert
were inerted, quiet parts which should have been active
were activated. The repaired cells were cultivated for
several more divisions; if they bred true, one or more of
them was returned to the original site—or at least, to
within a few microns of it. Cell division and tissue building
went on according to the modified plan until some new
discrepancy was detected.
Most of this was, of course, automatic; too many millions of operations were going on simultaneously for detailed manual control. Nevertheless, Mancini and Jellinge
were busy. Neither life nor pseudolife is infallible; mutations occur even in triply redundant records. Computation
errors occur even—or especially—in digital machines
which must by their nature work by successive-approximation methods. It is much better to have a human operator,
who knows his business, actually see that connective tissue
instead of epidermis is being grown in one spot, or nerve
instead of muscle cells in another.
Hence, a random selection of cells, not only from areas
which had aroused the computer’s interest but from those
where all was presumably going well, also traveled out
through the tubes. These went farther than just to the
incubators; they came out to a joint where gross microscopic study of them by a human observer was possible.
This went on twenty-four hours a day, the two mechanics
chiefly concerned and four others of their profession taking two-hour shifts at the microscope. The number of
man-hours involved in treating major bodily injury had
gone up several orders of magnitude since the time when a
sick man could get away with a bill for ten dollars from
his doctor, plus possibly another for fifty from his undertaker.
The tendrils and tubes farthest from the damaged tissue
were constantly withdrawing, groping their way to the
action front, and implanting themselves anew, guided by
the same chemical clues which brought leukocytes to the
same area. Early versions of the technique had involved
complex methods of warding off or removing the crowd of
white cells from the neighborhood; the present idea was to
let them alone. They were good scavengers, and the controller could easily allow for the occasional one which was
taken in by the samplers.
So, as days crawled by, skin and fat and muscle and
blood vessels, nerves and bones and tendons, gradually
extended into their proper places in Stubbs’ face and hand.
The face, as Mancini had predicted, was done first; the
severed hand had deteriorated so that most of its cells
needed replacement, though it served as a useful guide.
“Maybe I should have taken a new hand,” he said.
“With new prints I might have gotten away with a bank
robbery, and out short the time leading to my well-earned
retired leisure.”
“Don’t you believe it,” returned Mancini grimly. “Your
new prints would be on file along with your gene record
and retinal pattern back in Denver before I could legally
have unplugged you from the machine. I had to submit a
written summary of this operation before I could start,
even as it was. Forget about losing your legal identity and
taking up crime.”
“But it’s all right, Rick—the hand will be back in
service soon, and it shouldn’t take you many weeks to
learn to write with it again—”
“What?”
“It is a new set of nerves, remember. They’re connected
with the old ones higher up in your hand and arm, but
even with the old hand as a guide they probably won’t go
to exactly the same places to make contact with touch
transducers and the like. Things will feel different, and
you’ll have to learn to use a pen all over again.”
The AIR AutoDoc Independent Medical Treatment Center is a device in which the patient is placed in prone position. With probes and scanners, the AutoDoc will analyze the status of the patient and report same, along with suggested treatments which can be implemented. Supposedly "anyone" can operate the device, but Medical skills can aid the operator.
The 'Doc can diagnose and treat up to ten patients before resupply—purchase of a package of drugs and antitoxins at any "A" Starport of Tech Level 10 or better. This resupply includes examination by an electronic and computer technician and maintenance of equipment.
The AutoDoc can also act as a Low Berth to place critical patients in suspension until more complete treatment can be secured. The AutoDoc is capable of all of the following: accomplishing all types of first aid; minor operations such as appendectomies, suturing, and dental work; can be programmed for a specific environment or metabolism (new program tapes at 500 Imperial Credits each); has demonstrated a 72% reliability in diagnosing unusual diseases and viruses.
His arms were drawn out stiffly, and hurt; his feet and legs hurt too, and he couldn't move them, and there was this prickling at his brow. And he was blind.
No; his eyes were just closed. He opened them, and there was a white wall in front of him, patterned with a blue snow-crystal design, and he realized that it was a ceiling and that he was lying on his back. He couldn't move his head, but by shifting his eyes he saw that he was completely naked and surrounded by a tangle of tubes and wires, which puzzled him briefly. Then he knew that he was not on a bed, but on a robomedic, and the tubes would be for medication and wound drainage and intravenous feeding, and the wires would be to electrodes imbedded in his body for diagnosis, and the crown-of-thorns thing would be more electrodes for an encephalograph. He'd been on one of those things before, when he had been gored by a bisonoid on the cattle range.
"[Kenebuck] whistled, and something about the size of a small dog, but made of smooth, black metal, slipped out from behind a sofa nearby and slid on an aircushion over the carpeting to their feet. Ian looked down. It was a sort of satchel with an orifice in the top from which two metallic tentacles protruded slightly.
'A medical mech', he said.
'Yes,' said Kenebuck, 'cued to respond to the heartbeats of anyone in the room with it...Even if you killed me, this could get to me in time to keep it from being permanent...'"
"Who needs a real doctor when you got my machines and their scary needles?"—"Doctor" Zed's Med Vendor, BorderlandsIn The Future or sometime soon, you won't need a steady hand to heal people, some machine is already doing it for you. In a futuristic setting there will be machines that fix human bodies automatically. If a human doctor is participating in it at all, he will only press buttons and won't even touch a scalpel.The appearance of these machines can range from complex apparatus to seemingly magic circles.
Bacta tank from Star Wars: Episode V The Empire Strikes Back
A fond sci-fi wish is to grant human beings the same ability found in some animals: to re-grow amputated limbs and such. Traditionally this take the form of a medical tank the patient floats in, but sometimes it is genetically engineered as an innate ability.
In science fiction the concept dates back at least to 1939 in E. E. "Doc" Smith's Gray Lensman, but the idea dates back to the time when the first pre-human noticed those autotomy lizards that shed their tail and later re-grow them. In the late 1960s there was some science news about the amazing regeneration powers of newts, in 1969 Frank Herbert mentioned "Axolotl Tanks" in Destination: Void , Dune Messiah, and The God Makers. In the Herbert novels Axolotl Tanks are also used for human cloning.
PHILLIPS REGENERATION TREATMENT
“Come in, Kinnison,” Haynes invited. “Lacy wants to see you a minute, too. Doctor Phillips—Lensman Kinnison, Unattached. His name isn’t Phillips, of course; we gave him that in self-defense, to keep from trying to pronounce his real one.” Phillips, the Posenian, was as tall as Kinnison, and heavier. His figure was somewhat human in shape, but not in detail. He had four arms instead of two, each arm had two opposed hands, and each hand had two thumbs, one situated about where a little finger would be expected. He had no eyes, not even vestigial ones. He had two broad, flat noses and two toothful mouths; one of each in what would ordinarily be called the front of his round, shining, hairless head; the other in the back. Upon the sides of his head were large, volute, highly dirigible ears. And, like most races having the faculty of perception instead of that of sight, his head was relatively immobile, his neck being short, massive, and tremendously strong. “Right, my boy—surprisingly and pleasingly right!” Lacy exclaimed. “Why can’t you adopt that attitude, Haynes, and learn enough words so you can understand what a man’s talking about? But to reduce it to monosyllabic simplicity, Phillips is studying a thing that has baffled us for thousands of years. The lower forms of cells are able to regenerate themselves; wounds heal, bones knit. Higher types, such as nerve cells, regenerate imperfectly, if at all; and the highest type, the brain cells, do not do so under any conditions.” His old friend interrupted. “We got the idea perfectly. The question is, why can’t human beings repair nerves or spinal cords, or grow new ones? If such a worthless beastie as a starfish can grow a whole new body to one leg, including a brain, if any, why can’t a really intelligent victim of simple infantile paralysis—or a ray—recover the use of a leg that is otherwise in perfect shape?” “Phillips,” the Surgeon-Marshal began, “explain to this warhorse, in words of as few syllables as possible, what you are doing.” “The original problem was to discover what hormone or other agent caused proliferation of neural tissue…” “Wait a minute, I’d better do it,” Lacy broke in. “Besides, you wouldn’t do yourself justice. The first thing he found out was that the problem of repairing damaged nervous tissue was inextricably involved with several other unknown things, such as the original growth of such tissue, its relationship to growth in general, the regeneration of lost members in lower forms, and so on. You see, Haynes, it’s a known fact that nerves do grow, or else they could not exist; and in lower forms of life they regenerate. Those facts were all he had, at first. In higher forms, even during the growth stage, regeneration does not occur spontaneously. Phillips set out to find out why.” “The thyroid controls growth, but does not initiate it, he learned. This fact seemed to indicate that there was an unknown hormone involved—that certain lower types possess an endocrine gland which is either atrophied or non-existent in higher types. If the latter, it was no landing. He reasoned, however, since higher types evolved from lower, that the gland in question might very well exist in a vestigial state. He studied animals, thousands of them, from the germ upward. He exhausted the patience of the Posenian authorities; and when they cut off his appropriation, on the ground that the thing was impossible, he came here. We felt that if he were so convinced of the importance of the work as to be willing to spend his whole life on it, the least we could do would be to support him. We gave him carte blanche.” “The man is a miracle of perseverance, a keen observer, a shrewd reasoner, and a mechanic par excellence—a born researcher. So he finally found out what it must be—the pineal. Then he had to find the stimulant. Drugs, chemicals, the spectrum of radiation; singly and in combination. Years of plugging, with just enough progress to keep him at it. Visits to other planets peopled by races human to two places or more; learning everything that had been done along that line. When you fellows moved Medon over here (the Medonians made a giant FTL drive and drove the planet from Lundmark's Nebula to the Milky Way galaxy like it was a giant starship) he visited it as routine, and there he hit the jackpot. Wise himself is a surgeon, and the Medonians have had warfare and grief enough to develop the medical and surgical arts no end.” “They knew how to stimulate the pineal, but their method was dangerous. With Phillips’ fresh viewpoint, his wide-knowledge, and his mechanical genius, they worked out a new and highly satisfactory technique. He was going to try it out on a pirate slated for the lethal chamber, but von Hohendorff heard about it and insisted on being the guinea pig. Got up on his Unattached Lensman’s high horse and won’t come down. So here we are.” Haynes relented enough to let von Hohendorff go first, and both were given the necessary injections. The commandant was then strapped solidly into a chair; his head was immobilized with clamps. The Posenian swung his needle-rays into place; two of them, each held rigidly upon micrometered racks and each operated by two huge, double, rock-steady hands. The operator looked entirely aloof—being eyeless and practically headless, it is impossible to tell from a Posenian’s attitude or posture anything about the focal point of his attention—but the watchers knew that he was observing in microscopic detail the tiny gland within the old Lensman’s skull. Then Haynes. “Is this all there is to it, or do we come back for more?” he asked, when he was released from his shackles. “That’s all,” Lacy answered. “One stimulation lasts for life, as far as we know. But if the treatment was successful you’ll come back—about day after tomorrow, I think—to go to bed here. Your spare equipment won’t fit and your stumps may require surgical attention.” Sure enough, Haynes did come back to the hospital, but not to go to bed. He was too busy. Instead, he got a wheel-chair and in it he was taken back to his now boiling office. And in a few more days he called Lacy in high exasperation. “Know what you’ve done?” he demanded. “Not satisfied with taking my perfectly good parts away from me, you took my teeth too! They don’t fit—I can’t eat a thing! And I’m hungry as a wolf—I don’t think I was ever so hungry in my life! I can’t live on soup, man; I’ve got work to do. What are you going to do about it?” “Ho-ho-haw!” Lacy roared. “Serves you right—von Hohendorff is taking it easy here, sitting on top of the world. Easy, now, sailor, don’t rupture your aorta. I'll send a nurse over with a soft-boiled egg and a spoon. Teething—at your age—Haw-ho-haw!” “I had no idea, Admiral Haynes, that you… that there…” she paused. “That I was so much of a rebuild?” complacently. “Except in the matter of eyes—which he doesn’t need anyway—our mutual friend Kinnison has very little on me, my dear. I got so handy with the replacements that very few people knew how much of me was artificial. But it’s these teeth that are taking all the joy out of life. I’m hungry, confound it! Have you got anything really satisfying that I can eat?” And all this activity centered in one vast building and culminated in one man—Port Admiral Haynes, Galactic Councillor. And Haynes could not get enough to eat because he was cutting a new set of teeth! He cut them, all thirty two of them. Arm and leg, foot and hand grew perfectly, even to the nails. Hair grew upon what had for years been a shining expanse of pate. But, much to Lacy’s relief, it was old skin, not young, that covered the new limbs. It was white hair, not brown, that was dulling the glossiness of Haynes’ bald old head. His trifocals, unchanged, were still necessary if he were to see anything clearly, near or far. “Our experimental animals aged and died normally,” he explained graciously, “but I was beginning to wonder if we had rejuvenated you two, or perhaps endowed you with eternal life. Glad to see that the new parts have the same physical age as the rest of you—it would be mildly embarrassing to have to kill two Gray Lensmen to get rid of them.”
I stripped and backed into the clamshelled suit. The new ones were a hell of a lot more complicated, with all the new biometrics and trauma maintenance. But well worth the trouble of hooking up, in case you got blown apart just a little bit. Go home to a comfortable pension with heroic prosthesis. They were even talking about the possibility of regeneration, at least for missing arms and legs. Better get it soon, before Heaven filled up with fractional people. Heaven was the new hospital/rest-and-recreation planet.
These new ships were ugly as hell. Just an open framework with clamps to hold you in place, swiveled lasers fore and aft, small tachyon powerplants below the lasers. Everything automated; the machine would land us as quickly as possible and then zip off to harass the enemy. It was a one-use, throwaway drone. The vehicle that would come pick us up if we survived was cradled next to it, much prettier.
I wasn’t worried, of course. Abstractedly, I wished I hadn’t taken the pill.
“Prepare for ejection,” the machine’s female-mechanical voice said. “Five, four…”
The ship’s lasers started firing, millisecond flashes freezing the land below in jerky stroboscopic motion. It was a twisted, pockmarked jumble of fissures and random black rocks, a few meters below our feet. We were dropping, slowing.
“Three—” It never got any farther. There was a too-bright flash and I saw the horizon drop away as the ship’s tail pitched down—then clipped the ground, and we were rolling, horribly, pieces of people and ship scattering. Then we slid pinwheeling to a bumpy halt, and I tried to pull free but my leg was pinned under the ship’s bulk: excruciating pain and a dry crunch as the girder crushed my leg; shrill whistle of air escaping my breached suit; then the trauma maintenance turned on snick, more pain, then no pain and I was rolling free, short stump of a leg trailing blood that froze shiny black on the dull black rock. I tasted brass and a red haze closed everything out, then deepened to the brown of river clay, then loam and I passed out, with the pill thinking this is not so bad…
The suit is set up to save as much of your body as possible. If you lose part of an arm or a leg, one of sixteen razor-sharp irises closes around your limb with the force of a hydraulic press, snipping it off neatly and sealing the suit before you can die of explosive decompression. Then “trauma maintenance” cauterizes the stump, replaces lost blood, and fills you full of happy-juice and No-shock. So you will either die happy or, if your comrades go on to win the battle, eventually be carried back up to the ship’s aid station.
Forever War issue #5B from Titan Comics (2017) artwork by Steve Kurth
Finally I woke up in a regular bay. I was strapped down and being fed through a tube, biosensor electrodes attached here and there, but no medics around. The only other person in the little room was Marygay, sleeping on the bunk next to me. Her right arm was amputated just above the elbow.
I didn’t wake her up, just looked at her for a long time and tried to sort out my feelings. Tried to filter out the effect of the mood drugs. Looking at her stump, I could feel neither empathy nor revulsion. I tried to force one reaction, and then the other, but nothing real happened. It was as if she had always been that way. Was it drugs, conditioning, love? Have to wait to see.
One knock on the door and Dr. Foster barged in. He examined Marygay’s stump and then mine. He stuck thermometers in our mouths so we couldn’t talk. When he spoke, he was serious and blunt.
“I’m not going to sugarcoat anything for you. You’re both on happyjuice up to your ears, and the loss you’ve sustained isn’t going to bother you until I take you off the stuff. For my own convenience I’m keeping you drugged until you get to Heaven. I have twenty-one amputees to take care of. We can’t handle twenty-one psychiatric cases.
“Enjoy your peace of mind while you still have it. You two especially, since you’ll probably want to stay together. The prosthetics you get on Heaven will work just fine, but every time you look at his mechanical leg or you look at her arm, you’re going to think of how lucky the other one is. You’re going to constantly trigger memories of pain and loss for each other…You may be at each other’s throats in a week. Or you may share a sullen kind of love for the rest of your lives.
“Or you may be able to transcend it. Give each other strength. Just don’t kid yourselves if it doesn’t work out.”
They took the most severely wounded first, so it was several days before I went into surgery. Afterwards, I woke up in my room and found that they had grafted a prosthesis onto my stump, an articulated structure of shiny metal that to my untrained eye looked exactly like the skeleton of a leg and foot. It looked creepy as hell, lying there in a transparent bag of fluid, wires running out of it to a machine at the end of the bed.
An aide came in. “How you feelin’, sir?” I almost told him to forget the “sir” bullshit, I was out of the army and staying out this time. But it might be nice for the guy to keep feeling that I outranked him.
“I don’t know. Hurts a little.”
“Gonna hurt like a sonuvabitch. Wait’ll the nerves start to grow.”
“Nerves?”
“Sure.” He was fiddling with the machine, reading dials on the other side. “How you gonna have a leg without nerves? It’d just sit there.”
“Nerves? Like regular nerves? You mean I can just think ‘move’ and the thing moves?”
“’Course you can.” He looked at me quizzically, then went back to his adjustments.
What a wonder. “Prosthetics has sure come a long way.”
“Pross-what-ics?”
“You know, artificial—”
“Oh yeah, like in books. Wooden legs, hooks and stuff.”
How’d he ever get a job? “Yeah, prosthetics. Like this thing on the end of my stump.”
“Look, sir.” He set down the clipboard he’d been scribbling on. “You’ve been away a long time (a couple of hundred years, due to relativity). That’s gonna be a leg, just like the other leg except it can’t break.”
“They do it with arms, too?”
“Sure, any limb.” He went back to his writing. “Livers, kidneys, stomachs, all kinds of things. Still working on hearts and lungs, have to use mechanical substitutes.” The guy wasn’t kidding about the pain. And it wasn’t just the new leg, though that hurt like boiling oil. For the new tissues to “take,” they’d had to subvert my body’s resistance to alien cells; cancer broke out in a half-dozen places and had to be treated separately, painfully.
I was feeling pretty used up, but it was still kind of fascinating to watch the leg grow. White threads turned into blood vessels and nerves, first hanging a little slack, then moving into place as the musculature grew up around the metal bone.
I got used to seeing it grow, so the sight never repelled me. But when Marygay came to visit, it was a jolt—she was ambulatory before the skin on her new arm had started to grow; looked like a walking anatomy demonstration. I got over the shock, though, and she eventually came in for a few hours every day to play games or trade gossip or just sit and read, her arm slowly growing inside the plastic cast. I’d had skin for a week before they uncased the new leg and trundled the machine away. It was ugly as hell, hairless and dead white, stiff as a metal rod. But it worked, after a fashion. I could stand up and shuffle along. They transferred me to orthopedics, for “range and motion repatterning”—a fancy name for slow torture. They strap you into a machine that bends both the old and new legs simultaneously. The new one resists.
Shed Garvey, the medical tech, was hunched over his lab table, debriding the stump of Cameron Paj’s left
arm, when Holden walked in. A month earlier, Paj had gotten his elbow pinned by a thirty-ton block of ice
moving at five millimeters a second. It wasn’t an uncommon injury among people with the dangerous job of
cutting and moving zero-g icebergs, and Paj was taking the whole thing with the fatalism of a professional.
Holden leaned over Shed’s shoulder to watch as the tech plucked one of the medical maggots out of dead tissue (do not Google this unless you have a strong stomach. The same goes for Googling "debriding"). "What’s the word? " Holden asked. "It's looking pretty good, sir," Paj said. “I've still got a few nerves. Shed’s been tellin' me about how the
prosthetic is gonna hook up to it.” “Assuming we can keep the necrosis under control,” the medic said, “and make sure Paj doesn't heal up too
much before we get to Ceres. I checked the policy, and Paj here’s been signed on long enough to get one with
force feedback, pressure and temperature sensors, fine-motor software. The whole package. It'll be almost as
good as the real thing. The inner planets have a new biogel that regrows the limb, but that isn’t covered in our medical plan.” "F**k the Inners, and f**k their magic Jell-O. I'd rather have a good Belter-built fake than anything those
bastards grow in a lab. Just wearing their fancy arm probably turns you into an a**hole,” Paj said. Then he added
"Oh, uh, no offense, XO.” “ None taken. Just glad we're going to get you fixed up, " Holden said.
“Tell him the other bit,” Paj said with a wicked grin. Shed blushed. “I've, ah, heard from other guys who’ve gotten them," Shed said, not meeting Holden’s eyes. "Apparently
there’s a period while you're still building identification with the prosthetic when (masturbation) feels just like
getting a hand job.” Holden let the comment hang in the air for a second while Shed’s ears turned crimson. “Good to know,” Holden said. “And the necrosis?” "There's some infection. " Shed said. “The maggots are keeping it under control, and the inflammation’s
actually a good thing in this context, so we're not fighting too hard unless it starts to spread.”
“Is he going to be ready for the next run?” Holden asked. For the first time, Paj frowned. “S**t yes, I’ll be ready. l’m always ready. This is what I do, sir." “Probably,” Shed said. Depending on how the bond takes. If not this one, the one after. " "F**k that," Paj said. “I can buck ice one-handed better than half the skags you've got on this b**h." “Again,” Holden said, suppressing a grin, "good to know. Carry on.”
At the I-A medical center, the oval crechepod containing Orne's flesh dangled from ceiling hooks in a private room.
There were humming sounds in the dim, watery green of the room, and rhythmic chuggings, sighings, clackings. Occasionally, a door opened quietly and a white-clad figure would enter, check the graph tapes on the crechepod's instruments, examine the vital connections, then depart.
In the medical euphemism, Orne was lingering.
He became a major conversation piece at the interns' rest breaks: 'That agent who was hurt on Sheleb, he's still with us.'
'Man, they must build those guys different from the rest of us!'
'... Yeah. I heard he only has about one-eighth of his insides — liver, kidneys, stomach, all gone … Lay you odds he doesn't last out the month … Look at what old sure-thing Tavish wants to bet on!'
On the morning of his eighty-eighth day in the crechepod, the day nurse entered Orne's room for her first routine check.
She lifted the inspection hood, looked down at him. The day nurse was a tall, lean-faced professional who had learned to meet miracles and failures with equal lack of expression. She was just here to observe.
The daily routine with the dying (or already dead) I-A operative had lulled her into a state of psychological unpreparedness for anything but closing out the records. Any day now, poor guy, she thought.
Orne opened his only remaining eye and she gasped as he said in a low whisper: 'Did they clobber those dames on Sheleb?'
'Yes, sir!' the day nurse blurted. 'They really did, sir!'
'Another damn mess,' Orne said. He closed his eye. His breathing-simulation deepened and heart-demand increased.
The nurse rang frantically for the doctors.
Orne began to show small but steady signs of recovery. Within a month, the medics ventured an intestinal transplant which increased his response rate. Two months later, they placed him on an atlotl/gibiril regimen, forcing the energy transfer which allowed him to regrow his lost fingers and eye, restore his scalp line and erase the other internal-external damage.
Fourteen months, eleven days, five hours and two minutes after he had been picked up on Sheleb 'as good as dead', Orne walked out of the hospital on his own two legs, accompanied by an oddly silent Umbo Stetson.
Orne paused on the steps above the pad, breathed deeply of the chill air. 'Beautiful day,' he said. His new kneecap felt strange, a better fit than the old one. He was acutely conscious of all his new parts and the regrowth syndrome which made all crechepod graduates share the unjoke label of 'twice-born'.
So I lay there in the tank and craned my neck to see how the foot was growing. The regenerator fluid is thick, yellowish, and murky, but I could see I'd already sprouted a neat bunch of tarsal bones, coated with a misty jelly where the flesh was starting to creep back over them. The fluid filled my mouth and nostrils and lungs, which no doubt were healing at a good rate. The only real quarrel I've got with this death-and-regeneration business is that it's boring: even for fiddling little injuries the process can take hours. Once I was cut not so neatly in half by a riot-gun and spent five whole days growing a new me, from the belly down, like some stupid flatworm. Learning to die and live again is a necessary thing, though. Like they told us on the induction course, deep down in all our genes we've got this locked-in program that shrieks survival when death's about, and shrieks it so loud that you can't hear your other thoughts. Only way to stop that and get efficient is to get used to dying … and then, maybe, you can start thinking about promotion.
That one had been my forty-sixth death. I reckoned I was used to it.
They let me out of the sickbay in the end, after all the usual unpleasantness (lying there in the tank is dreamy and nice if you can turn off your brain awhile, but being disconnected isn't so good). I marched off on my own two tender feet — the treatment leaves you uncalloused, like a baby — feeling ready to rush that laser again and this time smear the crew good and proper. I'd been in some of those bunkers myself, of course. Sooner or later the crew always get smeared.
"Extraordinary," Ngabe muttered as he worked me over. "I very rarely have the opportunity to study patients resuscitated by tissue regeneration ... the technique is used only sparingly in my country, we have such problems of birthrate, alas … Yes, I feel I could have predicted the characteristic complexion, the atypical callousing … Of course this mole can have no malignant tendencies?"
"No. None. We don't talk about that much," I mumbled. That was one of the risks, you get a few rogue cells multiplying and, well, it had happened to my big-mouthed drinking buddy Hoare in the tank next to mine once. Hard to forget waking up from a night of regrowth, turning your head to say "Hi there" and finding something man-sized but quite shapeless in the tank next door. The thing had been still alive, they said. I don't know what they did with it.
The third time was the worst, but it was a familiar sort of worst. The jointed arms of the tank machinery whipped a plastic film around my head; the needle went into my arm to "partly de-inhibit the coughing reflex" (Mk III Regeneration Module: Subjects' Manual, p. 64). Air hissed into the bubble and the tank waited patiently while I coughed my lungs out and the bubble's outlet tube sucked away the gobs of yellow nastiness I spewed through mouth and nostrils. Starting to breathe again just isn't a nice business: it took something like an hour for me to settle down and live in the ordinary way, chest hurting like hell. Through the plastic bubble I could see, in a distorted fishbowl view, that the rest of me was safely there as I remembered it.
A week in the tank was big bad medicine. I'd only known one guy stay in longer, and he could never think straight afterward. But physically, I guessed, we'd been smashed up more than he had — perhaps we'd been in longer than a week, two weeks, three weeks? It was too late to ask how much of a rebuild job either of us was now, how much nonessential muscle and bone had been shoveled into disposal drums back at Tunnel — like the whiskery old Force gag about how to lose ten pounds of unsightly fat. The fluid was a kind of liquid flesh matrix, it said in the manual, and it could replace one hell of a lot.
Decontamination
artwork by Jeff Miller / Red Republik click for larger image
From Space: 1999. Wall label over Commander Konig's shoulder reads "Air Lock Decontamination Procedure"
If your ship may be boarding people who are infected with a deadly plague, malignant alien parasites, covered in dangerous chemicals, crawling with combat nanotechnology, or dusted with radioactive fallout, you probably do not want them getting your ship or crew dirty. A special airlock leading into a decontamination chamber would be in order.
This is a specialized feature not found on all ship types. You'd expect it on hospital ships, rescue ships, exploration ships, and ships bringing emergency supplies to planetary disaster sites.
A less effective but cheaper option is to use a "suitport". This is where a special space suit attaches its backpack to a hatch on the ship, and the astronaut exist the suit through the backpack. It does reduce, for instance, the external skin of the suit from transporting abrasive lunar dust contamination into the airlock. But the contamination on the backpack still has to be dealt with. A more serious problem is the pressure difference habitat module and the space suit.
Suitport
Suitport
In H. Beam Piper's Uller Uprising, the atmosphere of the planet was highly toxic to humans (large amounts of fluorine and fluoride gasses). The pressurized human bases and vehicles had special airlocks, with three consecutive chambers and four doors. Only one door would open at a time, and the middle chamber was always in vacuum. The purpose was to minimize traces of the planetary atmosphere entering the pressurized base.
Tail of "Hot" Suit Serves as Entrance
A technician puts on this plastic protective suit by crawling into it through its fat "tail," which is connected to a port in the door. Used in radioactive areas of the Hanford plutonium factory, it stays inflated because the air pressure inside the "hot" room is lower than pressure outside. This prevents any radioactive dust from leaking outside the room
Note long elastic tunnel attached to the back, leading to the hatch in the wall
click for larger image
In the novel and movie The Andromeda Strain at the top-secret underground Wildfire biological laboratory the doctors had to remove and burn their clothing, bathe in various chemical disinfectants, be exposed to ultraviolet rays, and have a xenon-flash unit burn the outer layer of skin and all their body hair into ash (except for the head). Oh, and rectal suppositories in a futile attempt to ensure that anal leakage was as sterile as possible.
The Wildfire laboratory also had something akin to a suitport but it was more like a glove-box. Except instead of covering just your hands, it covered your entire body. Like the Hanford suits, they had a long elastic tunnel attached to the back, leading to a hatch in the wall.
The Andromeda Strain
The Wildfire full-body glovebox. The baby and the old man are quarantined as they are infected with the deadly extraterrestrial Andromeda Strain. The two glove-suits are on the wall at left and right.
The Andromeda Strain
The glove-suits, with elastic tunnel attached to the back.
Through the window you can see the wall hatch
The Andromeda Strain
After ensuring that the glove-suit does not have a leak (which would make it full of deadly plague germs), the hatch is opened
The Andromeda Strain
Grabbing the upper rim of the hatch, the operator jumps through the tunnel and into the suit. The hatch slams shut behind the operator, just in case the suit springs a leak.
When the operator wants to exit, a control on the hatch will open it. Unless the suit's integrity has been compromised, in which case the control does absolutely nothing.
The Andromeda Strain
The operator removes the helmet ring on the top from the dangling hook. By moving forwards, the series of tunnel support wires moves along the suspension system in the ceiling. The system is a long bar that pivots left and right where it attaches to the wall
The Andromeda Strain
Naturally the decontamination method depends upon the expected contaminant.
Also note that the decontamination only removes surface contamination. If the people have internal contamination (infected by plague or inhaling radioactive fallout) they will have to be put into a quarantine chamber.
In the TV show Star Trek, they use the hand-waving Transporter to remove contamination, internal and external. As their atomic structure is removed from the starting location and transported to the ship, any (known) harmful bacterial, virus, or dangerous elements are "filtered out". Which is hand-waving at best and has creepy dystopian applications at worse.
THE ANDROMEDA STRAIN
1. THERE ARE TO BE FIVE STAGES:
Stage I: Non-decontaminated, but clean. Approximates sterility of hospital operating room or NASA clean room. No time delay of entrance.
Stage II: Minimal sterilization procedures: hexachlorophene and methitol bath, not requiring total immersion. One-hour delay with clothing change.
Stage III: Moderate sterilization procedures: total-immersion bath, UV irradiation, followed by two-hour delay for preliminary testing. Afebrile infections of UR and GU tracts permitted to pass. Viral symptomatology permitted to pass.
Stage IV: Maximal sterilization procedures: total immersion in four baths of biocaine, monochlorophin, xantholysin, and prophyne with intermediate thirty-minute UV and IR irradiation. All infection hafted at this stage on basis of symptomatology or clinical signs. Routine screening of all personnel. Six-hour delay.
Stage V: Redundant sterilization procedures: no further immersions or testing, but destruct clothing x2 per day. Prophylactic antibiotics for forty-eight hours. Daily screen for superinfection, first eight days.
They began at a door, which said in plain white letters: TO LEVEL II. It was an innocuous, straightforward, almost mundane sign. Hall had expected something more — perhaps a stern guard with a machine gun, or a sentry to check passes. But there was nothing, and he noticed that no one had badges, or clearance cards of any kind.
He mentioned this to Stone. “Yes,” Stone said. “We decided against badges early on. They are easily contaminated and difficult to sterilize; usually they are plastic and high-heat sterilization melts them.”
The four men passed through the door, which clanged shut heavily and sealed with a hissing sound. It was airtight. Hall faced a tiled room, empty except for a hamper marked ‘clothing’. He unzipped his jumpsuit and dropped it into the hamper; there was a brief flash of light as it was incinerated.
Then, looking back, he saw that on the door through which he had come was a sign: “Return to Level I is NOT Possible Through this Access.”
He shrugged. The other men were already moving through the second door, marked simply EXIT. He followed them and stepped into clouds of steam. The odor was peculiar, a faint woodsy smell that he guessed was scented disinfectant. He sat down on a bench and relaxed, allowing the steam to envelop him. It was easy enough to understand the purpose of the steam room: the heat opened the pores, and the steam would be inhaled into the lungs.
The four men waited, saying little, until their bodies were coated with a sheen of moisture, and then walked into the next room.
Leavitt said to Hall, “What do you think of this?”
“It's like a goddam Roman bath,” Hall said.
The next room contained a shallow tub (“Immerse Feet ONLY”) and a shower. (“Do not swallow shower solution. Avoid undue exposure to eyes and mucous membranes.”) It was all very intimidating. He tried to guess what the solutions were by smell, but failed; the shower was slippery, though, which meant it was alkaline. He asked Leavitt about this, and Leavitt said the solution was alpha chlorophin at pH 7.7. Leavitt said that whenever possible, acidic and alkaline solutions were alternated.
“When you think about it,” Leavitt said, “we've faced up to quite a planning problem here. How to disinfect the human body — one of the dirtiest things in the known universe — without killing the person at the same time. Interesting.”
He wandered off. Dripping wet from the shower, Hall looked around for a towel but found none. He entered the next room and blowers turned on from the ceiling in a rush of hot air. From the sides of the room, UV lights clicked on, bathing the room in an intense purple light. He stood there until a buzzer sounded, and the dryers turned off. His skin tingled slightly as he entered the last room, which contained clothing. They were not jumpsuits, but rather like surgical uniforms — light-yellow, a loose-fitting top with a V-neck and short sleeves; elastic banded pants; low rubber-soled shoes, quite comfortable, like ballet slippers.
The second decontamination procedure was similar to the first. Hall's yellow clothing, though he had worn it just an hour, was incinerated.
“Isn't that rather wasteful?” he asked Burton.
Burton shrugged. “It's paper.”
“Paper? That cloth?”
Burton shook his head. “Not cloth. Paper. New process.”
They stepped into the first total-immersion pool. Instructions on the wall told Hall to keep his eyes open under water. Total immersion, he soon discovered, was guaranteed by the simple device of making the connection between the first room and the second an underwater passage. Swimming through, he felt a slight burning of his eyes, but nothing bad.
The second room contained a row of six boxes, glass-walled, looking rather like telephone booths. Hall approached one and saw a sign that said, “Enter and close both eyes. Hold arms slightly away from body and stand with feet one foot apart. Do not open eyes until buzzer sounds. BLINDNESS MAY RESULT FROM EXPOSURE TO LONG-WAVE RADIATION.”
He followed the directions and felt a kind of cold heat on his body. It lasted perhaps five minutes, and then he heard the buzzer and opened his eyes. His body was dry. He followed the others to a corridor, consisting of four showers. Walking down the corridor, he passed beneath each shower in turn. At the end, he found blowers, which dried him, and then clothing. This time the clothing was white.
They dressed, and took the elevator down to Level III.
After two hours, he rejoined the others, and proceeded to Level IV.
Four total-immersion baths, three sequences of ultraviolet and infrared light, two of ultrasonic vibrations, and then something quite astonishing at the end. A steel-walled cubicle, with a helmet on a peg. The sign said, “This is an ultraflash apparatus. To protect head and facial hair, place metal helmet securely on head, then press button below.”
Hall had never heard of ultraflash, and he followed directions, not knowing what to expect. He placed the helmet over his head, then pressed the button.
There was a single, brief, dazzling burst of white light, followed by a wave of heat that filled the cubicle. He felt a moment of pain, so swift he hardly recognized it until it was over. Cautiously, he removed the helmet and looked at his body. His skin was covered with a fine, white ash — and then he realized that the ash was his skin, or had been: the machine had burned away the outer epithelial layers. He proceeded to a shower and washed the ash off. When he finally reached the dressing room, he found green uniforms.
“Decontamination complete, Milady! You may step through into the next cubicle and get dressed.”
Bethany watched the last of the vile smelling decontamination fluid gurgle down the drain at her feet, and then glanced up at the overhead speaker from which the unseen operator’s voice had emanated. As she did so, she wondered if he could see her.
“What about my clothing?” she asked, shivering slightly in the sudden cold draft of the chamber.
“Undergoing fumigation, Milady. You will find a new shipsuit in the cubicle.”
“Thank you!”
“You are most welcome.”
Bethany pressed the control that opened the airtight door leading from the chamber to the changing cubicle beyond. True to the operator’s word, the plastic bag into which she had sealed the clothing she had worn on Corlis was gone. In its place was a neatly folded replacement outfit. She dried herself, then carefully slipped into new underwear, shipsuit, and soft boots. She brushed her hair using a brush from the tiny personal effects kit that had accompanied the clothing, and studied the result in the full length mirror that hung on the inside of the cubicle door. Other than temporarily looking like a drowned rodent and smelling of disinfectant, she decided that she was none the worse for wear. She slipped the packet of personal effects into a pocket of the shipsuit, opened the cubicle door, and stepped into the corridor beyond.
“Welcome aboard Terra,” a voice said from somewhere behind her.
She turned to find Captain Lord Rheinhardt Dreyer, the Sandarian cruiser’s captain, waiting for her. The captain was a tall man, with a lean figure, close-cropped sandy hair, and eyes that were a pale blue. He wore the undress uniform of the Royal Sandarian Navy.
“Captain Dreyer! There was no need for you to come down to meet me.”
The Sandarian officer chuckled. “Oh, but there was. Captain Drake would have my ears if you were not treated properly while aboard my ship. I’m sorry that you couldn’t have been routed directly to Discovery, but the regulations concerning decontamination after a visit to an alien biosphere are extremely stringent.”
“As they should be,” Bethany replied. “I understand from Varlan that the Ryall had a number of laborers come down with unknown diseases on Corlis. I’m no expert, but it seems to me that any microorganism that can feed off Ryall biochemistry might do as well on human.”
(ed note: The Okie flying cities are sort of like FTL generation ships who are the migrant workers of space. The germanium monetary standard has unexpectedly crashed, so the entire blasted galaxy is suddenly broke. Amalfi, mayor of the flying city of New York, leads a boarding party into an apparently derelict flying city.)
The boarding-squad men deployed quickly along opposite sides of the street while the technics took cover. Amalfi sidled along the near wall to where the sergeant was crouching.
"What do you think, Anderson?"
"I don't like it, Mr. Mayor. It stinks of mouse traps. Maybe everybody's dead and the last man didn't have the strength to turn out the light. On the other hand, just one light left burning for that reason, in the whole city?"
"I see what you mean. Dulany, take five men down that side street where the facsimile pillar is, follow it until you're tangent to the corner of this building up ahead, and stick out a probe. Don't use more than a couple of micro-volts, or you might get burned."
"Yessir." Dulany's squad—the man himself might best be described as a detector-detector—slipped away soundlessly, shadows among shadows.
"That isn't all I stopped us for, Mr. Mayor," Anderson said. "There's a grounded aircab just around the corner here. It's got a dead passenger in it. I wish you'd take a look at him."
Amalfi took the proffered torch, covered its lens with the mitten of his suit so that only a thin shred of light leaked through and played it for half a second through the cab's window. He felt his spine going rigid. Wherever the light touched the flesh of the hunched corpse, it—glistened…
"Communications!"
"Yes, sir!" "Set up the return port for decontamination. Nobody gets back on board our town until he's been boiled alive—understand? I want the works."
There was a brief silence. Then: "Mr. Mayor, the city manager already has that in the works."
Amalfi grimaced wryly in the darkness. Anderson said, "Pardon me, sir, but—how did Mr. Hazleton guess?"
"Why, that's not too hard to see, at least after the fact, sergeant. This city we're on was desperately poor. And being poor under the new money system means being low on drugs. The end result, as Mr. Hazleton saw, and I should have seen, is—plague."
"The sons of bitches," the sergeant said bitterly. The epithet seemed intended to apply to every non-Okie in the universe.
 The one profession that is never out of a job is a good doctor (second most job secure is a good cook).
The one profession that is never out of a job is a good doctor (second most job secure is a good cook).